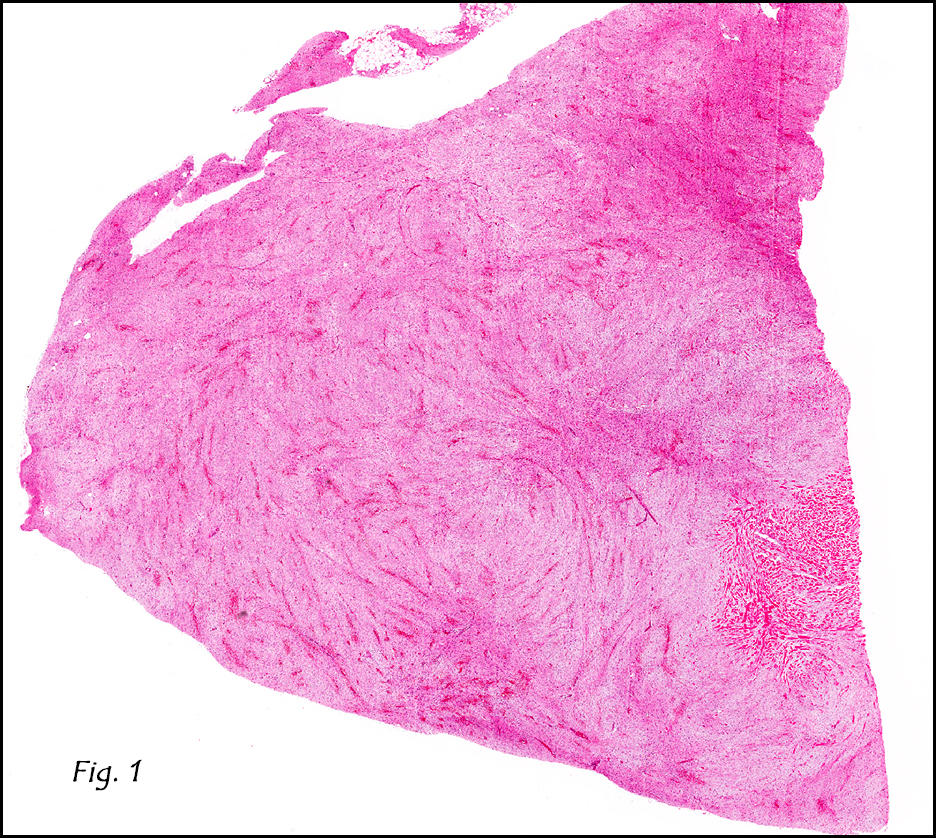
History: A 66-year-old male dwarf underwent surgical excision of a 6.0 cm mesenteric mass. The cut surface resembled white scar tissue.
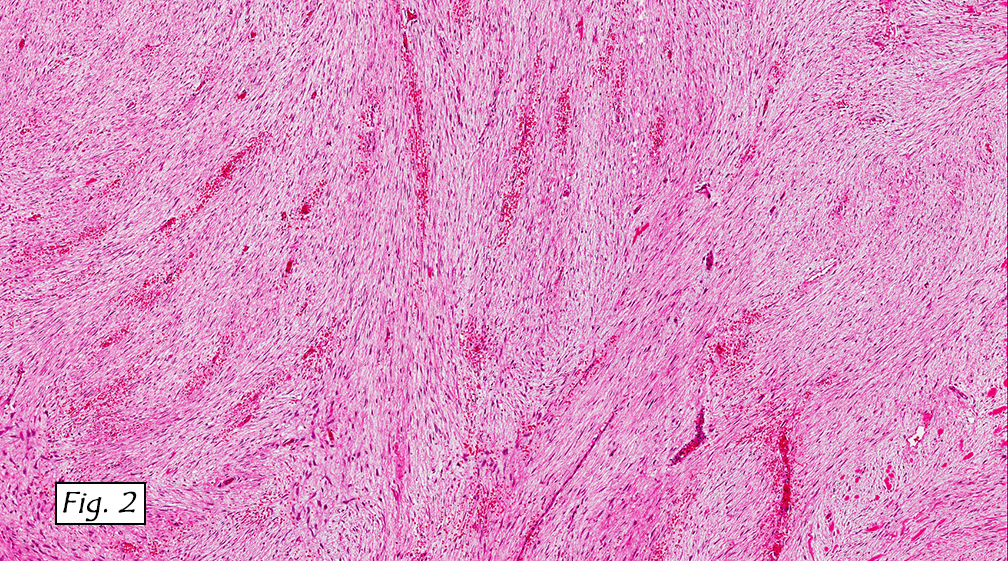
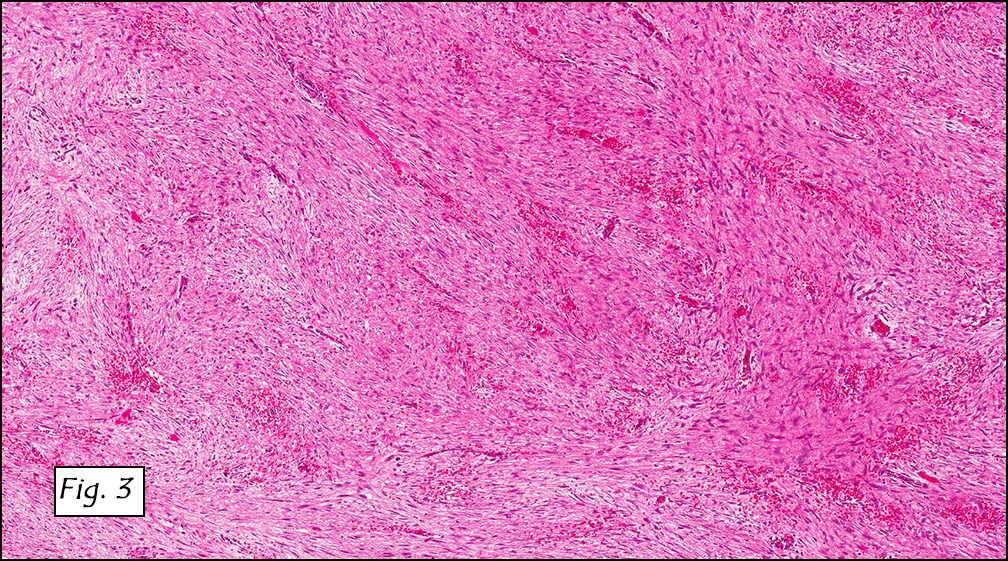
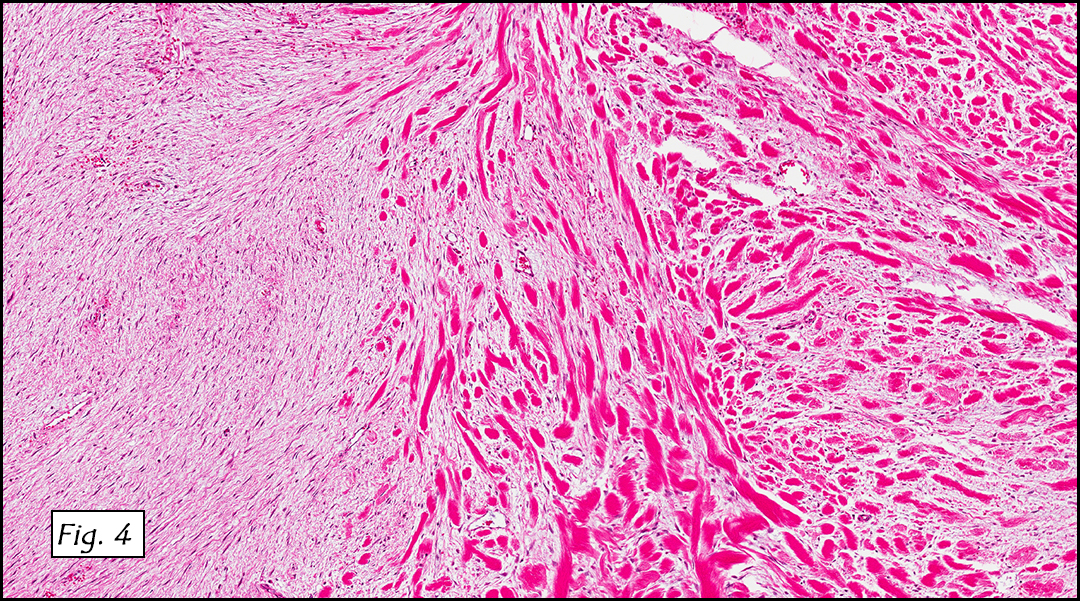
Microscopically, the mass was of fibrous tissue with prominent blood vessels (Fig. 1). Spindle-shaped cells were evenly spaced among mature collagen arranged in long sweeping fascicles (Fig. 2). The stroma showed variable density (Fig. 3) and there was an area which consisted of thick bundles of collagen (keloidal fibrosis), (Fig. 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Mesenteric Fibromatosisâ€
Matthew S. Johnson, PSF, and Donald R. Chase, MD
Department of Pathology & California Tumor Tissue Registry, Loma Linda University and Medical Center, Loma Linda, California
Discussion: Mesenteric fibromatosis (MF) is classified as an intra-abdominal fibromatosis, and one of a part of a larger group of fibromatoses that are microscopically similar. Fibromatoses in general are benign fibroproliferative processes that may demonstrate infiltrative growth but do not metastasize. Deep fibromatoses have about a 50% recurrence rate, and the superficial variants about 10%. MF accounts for a mere 8% of all fibromatosis cases. These tumors typically arise in the mesentery of the small bowel and the ileocecal region, but occasionally occur in the omentum and retroperitoneum. They usually present as asymptomatic abdominal masses or are found incidentally in patients of various ages (mean age of 41 years) and are more common in males. It is common for them to measure 10 cm or more. Grossly, they well-circumscribed, white masses that may be either soft or firm.
Histologically, MF is comprised of a dense collagenous stroma with evenly dispersed spindle or stellate cells and prominent blood vessels. The cellularity may be variable with stroma ranging from densely fibrous to markedly myxoid. Foci of keloidal fibrosis (thick collagen bundles) are a hallmark feature, present in approximately 50% of cases.
Immunohistochemical studies can help distinguish MF from other tumors. MF displays strong nuclear staining for β-catenin but is negative for CD117, CD34, and S-100.
Differential Diagnosis:
• Gastrointestinal stromal tumor (GIST) is the most common misdiagnosis. They usually have greater cellularity and atypia then do MFs. Also helping to distinguish are the keloidal fibrosis, infiltrative growth pattern, and prominent thin-walled blood vessels which are commonly found in MF but not in GIST. The tumors are also separated by their immunostaining patterns. GIST tends to be positive for CD117, CD34, and β-catenin, and MF is not.
• Sclerosing mesenteritis may also present as a large mass in the mesentery of small bowel, but the histological findings of fat necrosis, chronic inflammation, less fibrosis, and lack of β-catenin expression distinguish it, as does the negative CD 117.
• Inflammatory myofibroblastic tumor of the mesentery or retroperitoneum is a consideration, but usually shows increased cellularity, cytologic atypia, and a greater degree of inflammation. These may also be positive for ALK-1 protein.
• Idiopathic retroperitoneal fibrosis typically displays lymphoplasmacytic inflammation dispersed among bands of dense hyalinized collagen.
MF is associated with familial adenomatous polyposis (FAP), in fact fibromatosis is found in approximately 10 to 15% of patients with FAP and often develops within two years after surgical excision of the affected intestinal tract. Diligent post-operative observation in FAP patients and endoscopic examination of the bowel in MF patients without known FAP is warranted.
Local recurrence is common. Greater recurrence rates have been observed in patients with FAP (90%) versus those without (12%). Recurrent tumors in FAP patients also tend to behave more aggressively and respond worse to therapy. Treatment involves complete excision of the tumor, which is often complicated by intestinal attachment. Alternative therapeutic options including postoperative radiation, chemotherapy, and anti-estrogenic agents have shown mixed results.
Suggested Reading:
Rodriguez JA; Guarda LA; Rosai J. Mesenteric fibromatosis with involvement of the gastrointestinal tract. A GIST simulator: a study of 25 cases. Am J Clin Pathol 2004 Jan;121(1): p93-8.
Pai SA; Zaveri SS. Intra-abdominal fibromatosis of the jejunum and mesentery. J Clin Pathol 2004 Oct;57(10): p1119.
Montgomery E; Torbenson MS; Kaushal M; Fisher C; Abraham SC. Beta-catenin immunohistochemistry separates mesenteric fibromatosis from gastrointestinal stromal tumor and sclerosing mesenteritis. Am J Surg Pathol 2002 Oct;26(10): p1296-301.
Church J; Berk T; Boman BM; Guillem J; Lynch C; Lynch P; Rodriguez-Bigas M; Rusin L; Weber T. Staging intra-abdominal desmoid tumors in familial adenomatous polyposis: a search for a uniform approach to a troubling disease. Dis Colon Rectum 2005 Aug;48(8): p1528-34.
Holubar S; Dwivedi AJ; O’Connor J. Giant mesenteric fibromatosis presenting as small bowel obstruction. Am Surg 2006 May;72(5): p427-9.