History: A 44 year old man presented with a five year history of a left index finger nodule. It was mildly painful and had been increasing in size over the past year. The excised specimen was 1.2 x 0.7 x 0.4 cm and had a somewhat gritty firm, yellow tan cut surface.
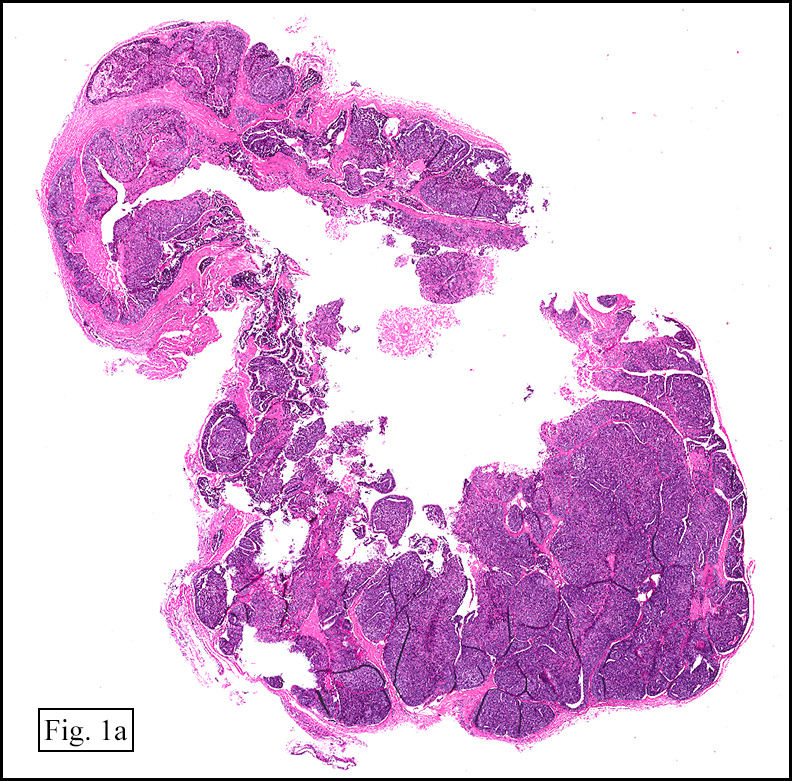
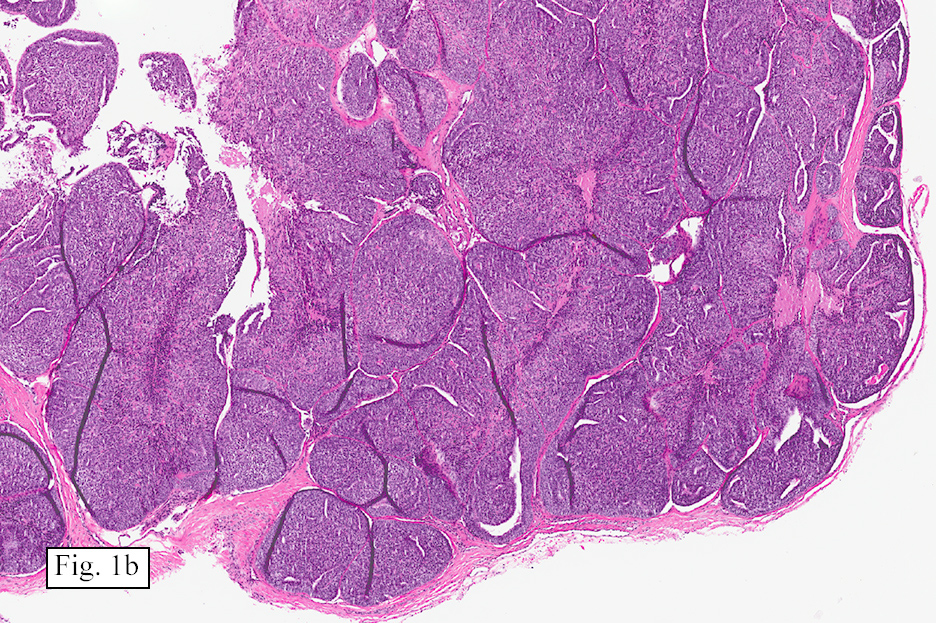
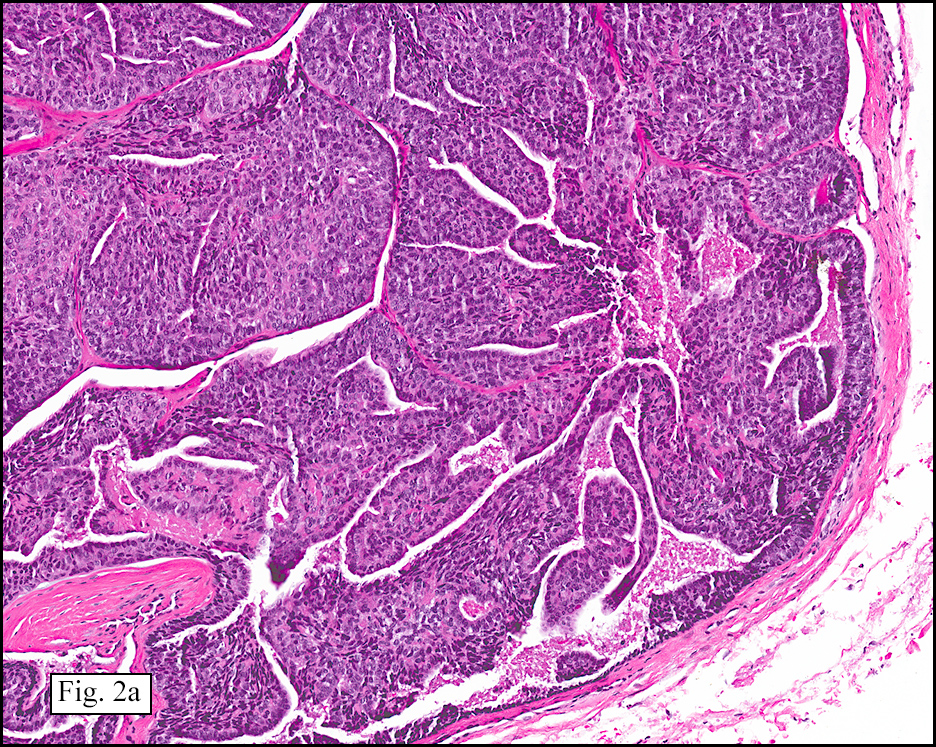
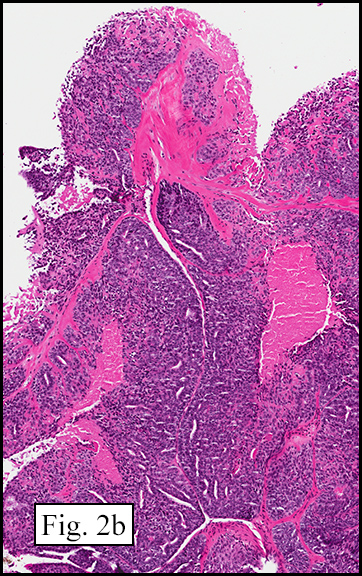
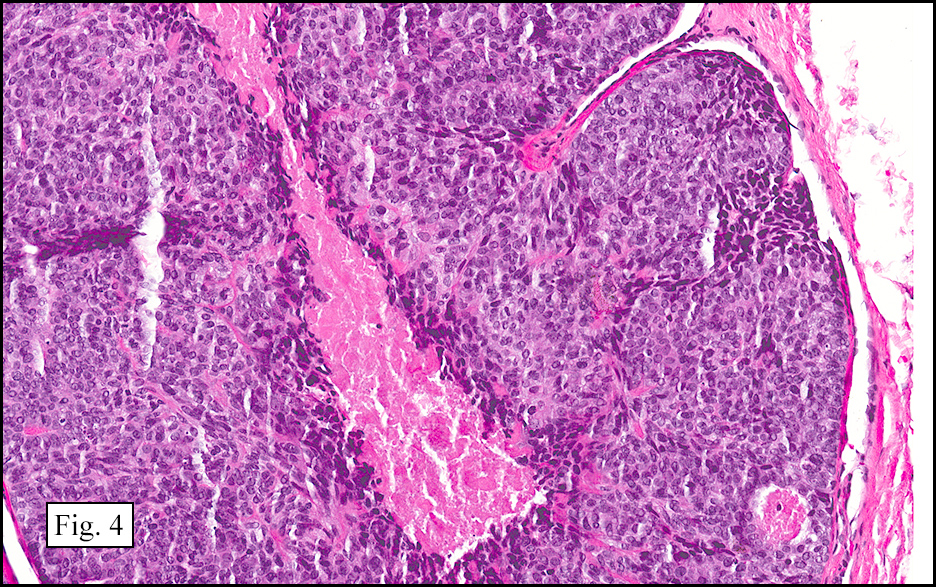
Microscopically, the tumor was cystic and well circumbscribed (Figs. 1a, 1b). There were papillary regions (Figs. 2a, 2b) with cells showing round to oval vesicular nuclei and cytologic atypia (Fig 3) Mitotic figures and necrosis were present (Fig. 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Aggressive Digital Papillary Adenocarcinoma
Dennis Aaron Reinke M.D. and Donald R. Chase, M.D.
Department of Pathology & Human Anatomy
Loma Linda University Medical center, Loma Linda, California
Discussion: Described by Dr. Helwig in 1977 as “Papillary eccrine adenomaâ€, the tumor was later renamed “Aggressive Digital Papillary Adenocarcinoma†(ADPA). It is felt to be of sweat gland origin and tends to occur in the digits, palms or soles. ADPA generally presents as a solitary nodule, usually 2 cm or larger and may be painful. The clinical suspicion is giant cell tumor of the tendon sheath, gout, soft tissue infection, pyogenic granuloma, glomus tumor, or ganglion cyst. Only rarely is there a history of trauma or chemical exposure. Most cases tend to occur in older men (males:females = 7:1) with a median age of 52 years, but it has been seen in ages as young as 14.
ADPA are usually cystic masses that involve the dermis and/or subcutis. They are often poorly circumscribed and infiltrative and microscopically show epithelial nodules that have papillary projections and glandular elements. The cells lining the cystic spaces may show atypia, pleomorphism and/or mitoses. The glandular cells can be cuboidal or columnar with round to oval vesicular nuclei. Necrosis may be present. The stroma is variable and may show areas of thin, fibrous septae or thick hyalinized collagen. Clear cell change, squamous metaplasia, and areas with spindle cells are sometimes seen. Most ADPAs are positive for keratin, carcinoembryonic antigen (CEA), and S-100 stains.
Fine needle aspiration cytology may be helpful for early diagnosis of ADPA. Syncytial groups with complex folded branching sheets of pleomorphic epithelial cells with clear anatomical borders are characteristic. There usually is nuclear overlap and crowding. Microscopically, fibrovascular cores may be seen having cells with large pale nuclei with finely granular chromatin and nucleoli. The cytoplasm is dense and cell borders are distinct.
ADPAs are known to locally recur, and metastasis is not uncommon. Studies on the rates of metastasis vary, but appear to range from 4-41.2%. The most common metastatic site is lung; however regional lymph nodes may also be involved.
Treatment of aggressive digital papillary adenocarcinoma should include wide excision or amputation of the digit at the appropriate level. One study suggested that patients receiving this treatment had ~5% likelihood of local recurrence; while those not treated with wide excision or amputation have ~50% chance of local recurrence.
Microscopically, the differential diagnosis includes:
• Aggressive papillary adenoma and aggressive papillary adenocarcinoma have previously been considered as distinct entities, based on criteria such as glandular differentiation, mitotic rate, necrosis, more pronounced cellular atypia, presence of zonal pleomorphism, and presence of bony or vascular invasion. However recent studies have suggested that since rates of metastasis and local recurrence are similar, they should be considered the same disease and treated the same.
• Papillary eccrine adenoma most often occurs in the distal extremities of African Americans. Tubular structures similar to eccrine ducts may often be dilated and contain intraluminal papillomata. Unlike ADPA they do not metastasize.
• Malignant eccrine acrospiromas are characterized by infiltrative architecture, perineural and lymphovascular invasion, atypical mitoses and pleomorphism. It may show solid, papillary, or glandular patterns and appear as a poorly differentiated adenocarcinoma. Atypical cells of ADPA may sometimes be seen next to the benign components of eccrine acrospiromas.
• Metastatic origin: Microscopically, aggressive papillary adenocarcinoma is usually not confused with other skin neoplasms, as the sites of involvement and papillary architecture of the lesions point to the diagnosis. It may however, appear very similar to other metastatic adenocarcinomas. A careful history and use of imaging studies should be pursued to rule out breast, lung, thyroid, ovarian, and other primary malignancy sites. Positive p63 expression tends to occur in primary lesions, while it is often negative in metastases.
In summary, aggressive papillary adenocarcinoma of the digit is a rare tumor that primarily involves tissues of the digits, palms or soles of men over age 50. They show a characteristic papillary cystic pattern with irregular and branching tubuloalveolar and ductal structures lined by epithelial cells that may show atypia, pleomorphism and mitoses. Appropriate identification is important to warrant aggressive surgical intervention to prevent local recurrence and metastasis.
Suggested Reading:
1. Altman CE, Hamill RL, Elston DM. Metastatic aggressive digital papillary adenocarcinoma. Cutis. 2003;72(2):145-7.
2. Holden B, Colome-Grimmer M, Savage C, Stierman K, Pou A. Malignant eccrine acrospiroma with metastasis to the parotid. ENT: Ear, Nose & Throat Journal [serial online]. May 2002;81(5):352.
3. Horii T, Sekiya H, Takatoku K, Hoshino Y. Aggressive digital papillary adenocarcinoma 5 years after surgical resection of adenoma on index finger. European Journal Of Orthopaedic Surgery & Traumatology [serial online]. July 2010;20(5):397-399.
4. Hsu H, Ho C, Chen C, Yang C, Hong H, Chuang Y. Aggressive digital papillary adenocarcinoma: a review. Clinical & Experimental Dermatology [serial online]. March 2010;35(2):113-119.
5. Krishnamurthy J, Patil, B. Aggressive digital papillary adenocarcinoma diagnosed by fine needle aspiration cytology. J Cytol. 2010 July;27(3):109-111.
6. Keramidas E, Miller G, Revelos K, Kitsanta P, Page R. Aggressive digital papillary adenoma-adenocarcinoma. Scandinavian Journal Of Plastic & Reconstructive Surgery & Hand Surgery [serial online]. June 2006;40(3):189-192.
7. Malafa M, Mckesey P, Stone S, Dudley-Walker S, Cockerell C. Sentinel Node Biopsy for Staging of Aggressive Digital Papillary Adenocarcinoma. Dermatologic Surgery [serial online]. June 2000;26(6):580-583.
8. McKee PH, Calonje E, Granter SR. Pathology of the Skin, With Clinical Correlations. [Edinburgh] : Elsevier Mosby, c2005.; 2008:1631-1632.
9. Rosai J, Ackerman LV. Rosai and Ackerman’s Surgical Pathology. Mosby; 2011:138-142.
10. Suchak R, Wang WL, Prieto VG, et al. Cutaneous digital papillary adenocarcinoma: a clinicopathologic study of 31 cases of a rare neoplasm with new observations. Am J Surg Pathol. 2012;36(12):1883-91.
11. Courtiss EH, Ruin DB, Helwig EB. Papillary eccrine adenoma. Plast Reconstr Surg. 60(6), 1977.
12. Duke WH, Sherrod TT, Lupton GP. Aggressive digital papillary adenocarcinoma (aggressive digital papillary adenoma and adenocarcinoma revisited). Am J Surg Pathol 2000 24(6):775-84.
13. Kao GF, Graham JH, Helwig EB. Aggressive digital papillary adenoma and adenocarcinoma. Arch Dermatol. 1984;120:1612.
14. Kao GF, Helwig EB, Graham JH. Aggressive digital papillary adenoma and adenocarcinoma. A clinicopathological study of 57 patients with histochemical, immunological and ultrastructural observations. J Cutan Pathol. 1987;14:129-146.