History: A 60 year-old woman presented with a progressively enlarging, deeply-seated mass in her right thigh. A 4.5 x 3.5 x 3.0 cm, well-circumscribed, nodular, soft tissue mass was excised.
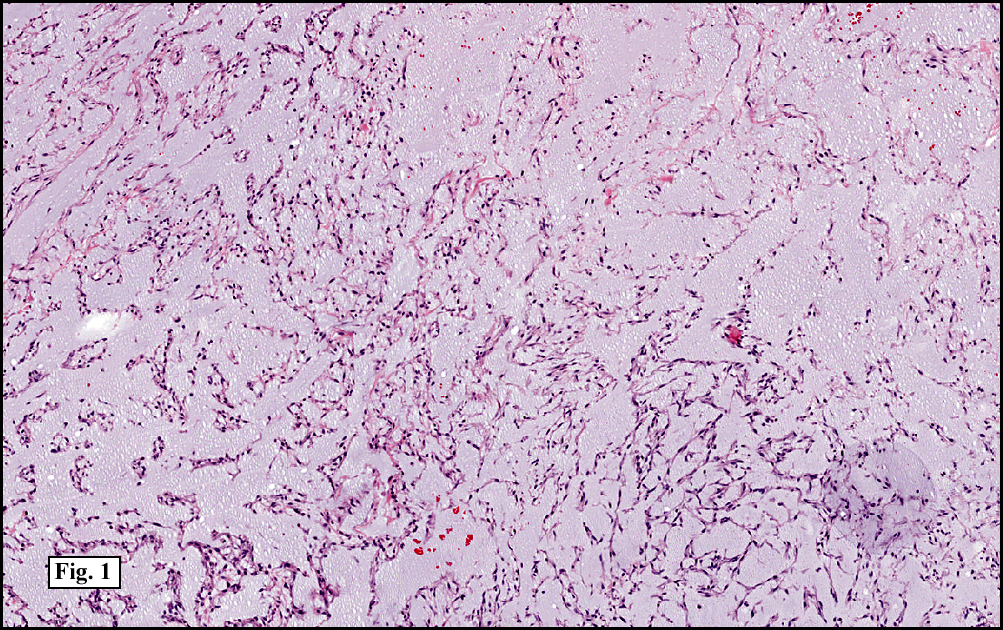
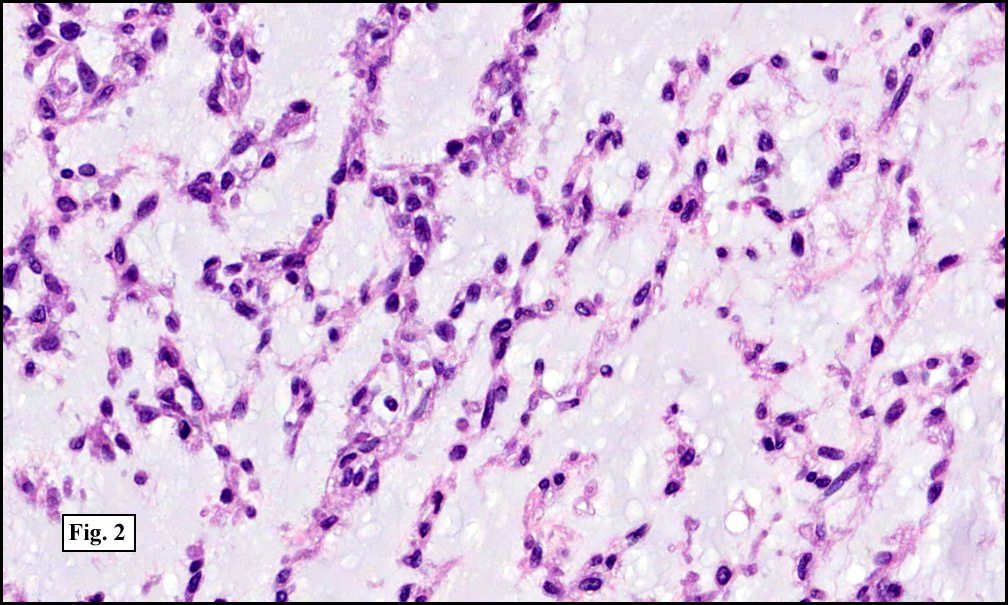
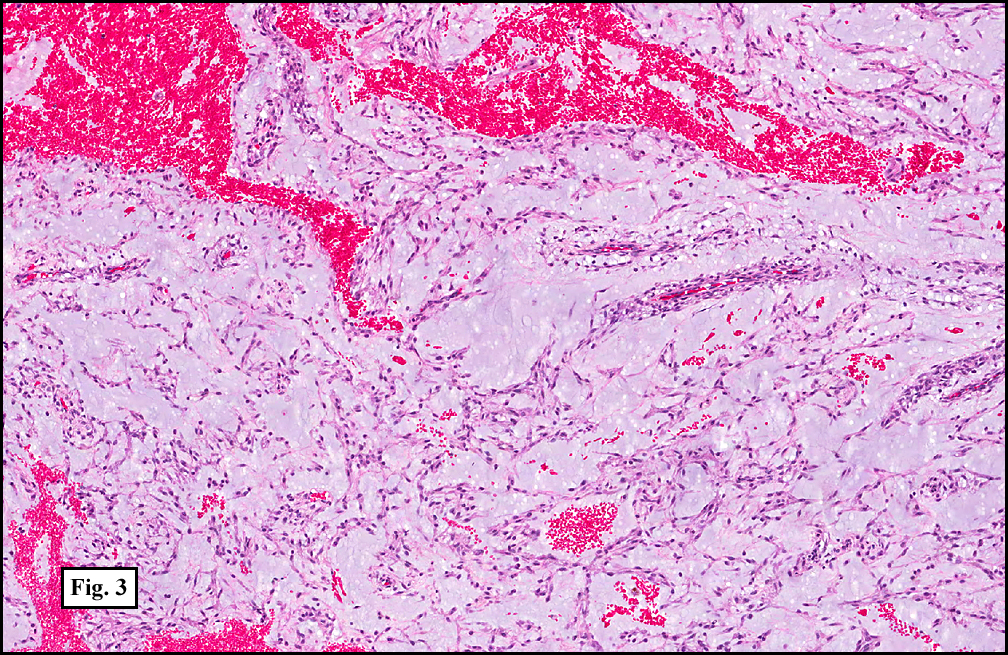
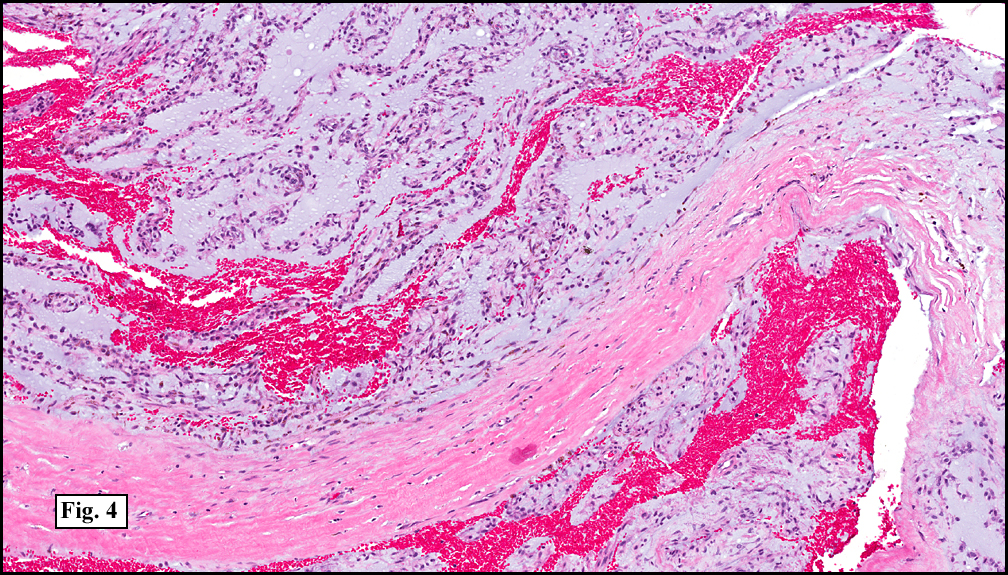
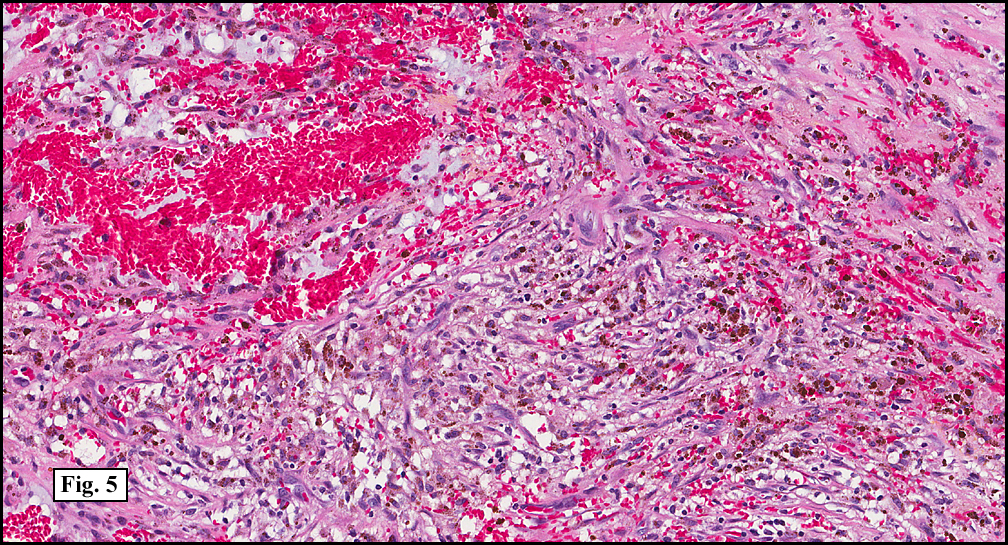
Microscopically, the tumor was composed of small eosinophilic cells with round to oval nuclei arranged in strands and cords separated by an abundant myxoid matrix (Fig. 1, 2). There were varying degrees of cellularity, ranging from areas with high cellularity and a vaguely storiform pattern to paucicellular areas with stellate, tissue culture-like cells embedded in a thick myxoid background (Fig. 3). Focal bands of mature collagen were seen (Fig. 4, at times, associated with copious hemorrhage and hemosiderin deposition (Fig. 5.). Mitotic figures were difficult to identify.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical staining was performed to exclude other possible mimicking lesions. The tumor did not stain for S100 protein, cytokeratins, or desmin; ruling out a tumor of melanocytic/neural, epithelial, or myogenic derivation, respectively.
Diagnosis: “Extraskeletal Myxoid Chondrosarcomaâ€
Brian Willis PSF and Donald Chase MD
Department of Pathology, Loma Linda University and Medical Center,
Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Extraskeletal myxoid chondrosarcoma (EMC) is a rare morphologically unique malignant soft tissue sarcoma characterized by cords and strands of chondroblast-like cells deposited in an abundant myxoid matrix. Although the nomenclature suggests cartilaginous differentiation, this tumor is currently classified as a tumor of uncertain differentiation due to the lack of convincing evidence that the cells represent actual chondroblasts.
EMC usually arises in the deep tissues of the proximal extremities and limb girdles of adults, primarily during the fifth and six decades, with only a few rare cases encountered in children and adolescents. Men are affected nearly twice as often as women. It has a predilection to develop in the thigh or popliteal fossa, similar to myxoid liposarcoma; however, rare examples of other unusual locations have been reported. Clinical symptoms are non-specific, with most patients presenting with a slowly growing deep-seated mass that may cause pain and tenderness. Radiographic findings are not distinctive; however, it should be noted that because a morphologically identical tumor may occur in bone and correlation with MRI or CT findings are necessary to establish soft tissue origin.
Grossly, conventional EMC is a circumscribed multinodular mass surrounded by a dense fibrous pseudocapsule. Sectioning reveals a gelatinous tan-brown surface divided into lobules by thick fibrous septa, frequently with large amounts of hemorrhage. Most tumors are 4-7 cm in greatest diameter at the time of resection, however, tumor sizes ranging from 1.1 to 25.0 cm have been reported.
Histologically, the tumor consists of nodules of uniform elongated cells in anastamosing cords and strands embedded in an abundant myxoid matrix separated by dense fibrous septa. These cells have small hyperchromatic nuclei with a rim of deeply eosinophilic cytoplasm which may resemble chondroblasts; however, unlike osseous chondrosarcomas there is no differentiation towards cartilage producing cells, and distinct chondrocytes in lacunae are never encountered. Other less common patterns that have been reported include a pseudoacinar pattern and a “cellular variant†with sheets of epithelioid cells with vesicular nuclei reminiscent of Ewings sarcoma. Mitotic figures are rare in most cases, but may be more abundant in undifferentiated cellular forms of the tumor.
Immunohistochemical findings are essentially non-contributory, with positivity for vimentin being the only consistent marker. Varying results have been obtained using S-100 protein, with reports ranging from about 18-40% positivity. In addition, scattered, focal reactivity to keratins and EMA, as well as synaptophysin and neuron-specific enolase have been reported in some cases.
The ultrastructural features are consistent mesenchymal origin, and in some cases feature intracisternal microtubules, a distinct finding that is also present in cases of myxoid chondrosarcoma of the bone. The cytoplasm and rough endoplasmic reticulum contain inclusions of granular material identical to that found in the extra cellular matrix.
EMC is characterized by several distinct cytogenetic findings. The most common and unique clonal abnormality is a balanced translocation t(9;22)(q22;q12) which results in the fusion of the EWS gene on 22q12 with the NR4A3 gene on 9q22. A second less common, but equally specific, translocation t(9;17)(q22;q12) fuses NR4A2 with RBP56. While the molecular consequence of these translocations has yet to be fully elucidated, it appears that the RBP56 and EWS fusion proteins have almost identical oncogenic potential. In a recent study, Filion and colleagues demonstrated that the EWS/NR4A3 fusion protein upregulates the nuclear PPARG gene.
The differential diagnosis of extraskeletal myxoid chondrosarcoma includes:
• Chondroid syringoma
• Parachordoma
Chondroid syringoma is a benign tumor of the skin and subcutaneous tissue that typically occurs in the head and neck. This tumor is of epithelial derivation but features large areas of myxoid stroma with chondrocyte-like cells. It is distinguished from EMC by the presence of duct like structures lined with a two cell layer that stain strongly positive for cytokeratins.
Parachordoma is an unusual entity of uncertain type that may represent a part of a morphologic spectrum that includes myoepithelioma of soft tissue and mixed tumor. This tumor may form lobules with nests of spindled cord-like cells in a myxoid matrix, mimicking the some of the histological findings of EMC; however, it is distinguished by its consistent co-expression of S-100 protein and cytokeratins. Further cytogenetic studies to demonstrate the characteristic t(9,22) translocations of EMC may be of value in particularly difficult cases.
Extraskeletal myxoid chondrosarcoma is a slow-growing tumor that is prone to late local recurrence and may eventually metastasize. While a possibly aggressive clinical course may be suggested by the findings of high grade or cellular variants, the results of large studies fail to correlate cellularity with prognosis. It is therefore, most prudent to treat all suspected cases of extraskeletal myxoid chondrosarcoma with radical local excision with or without adjuvant high-dose radiation to prevent the possibility of future local recurrence.
Suggested Reading:
1. Enzinger FM, Shiraki M. Extraskeletal myxoid chondrosarcoma. An analysis of 34 cases. Hum Pathol 1972; 3: 421-435
2. Meis-Kindblom JM, Bergh P, Gunterberg B, Kindblom LG. Extraskeletal myxoid chondrosarcoma: a reappraisal of its morphologic spectrum and prognostic factors based on 117 cases. Am J Surg Phathol 1999; 23: 636-650
3. Subramanian S, West R B, Marinelli RJ, et al. The gene expression profile of extraskeletal myxoid chondrosarcoma. J Pathol 2005; 206: 433-444
4. Fletcher CD M, Powell G, Mckee PH. Extraskeletal myxoid chondrosarcoma: a histochemical and immunohistochemical study. Histopathology 1986; 10: 489-499
5. Drilon AD, Popat S, Bhuchar G, et al. Extraskeletal myxoid chondrosarcoma: a retrospective review from 2 referral centers emphasizing long-term outcomes with surgery and chemotherapy. Cancer 2008; 113(12): 3364-3371
6. Filion C, Motoi T, Olshen AB, et al. The EWSR1/NR4A3 fusion protein of extraskeletal myxoid chondrosarcoma activates the PPARG nuclear receptor gene. J Pathol. 2009; 217(1): 83-93