History: A 76-year-old female presented with a two week history of a 7.1 cm nodular tumor in the buttock. It was violaceous, raised and firm. There was also adenopathy in the groin.
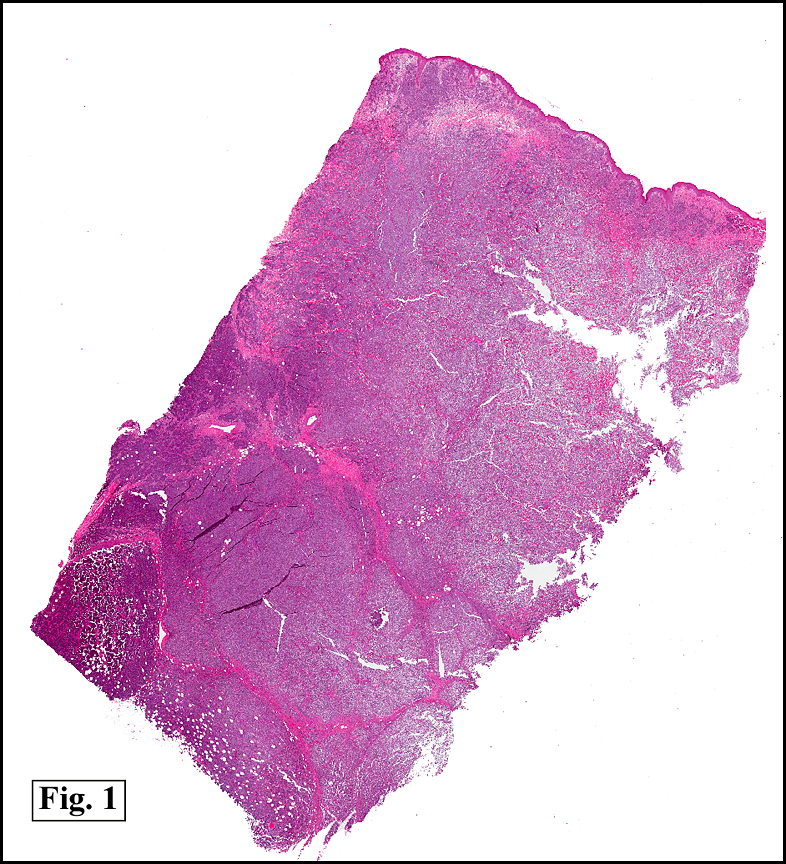
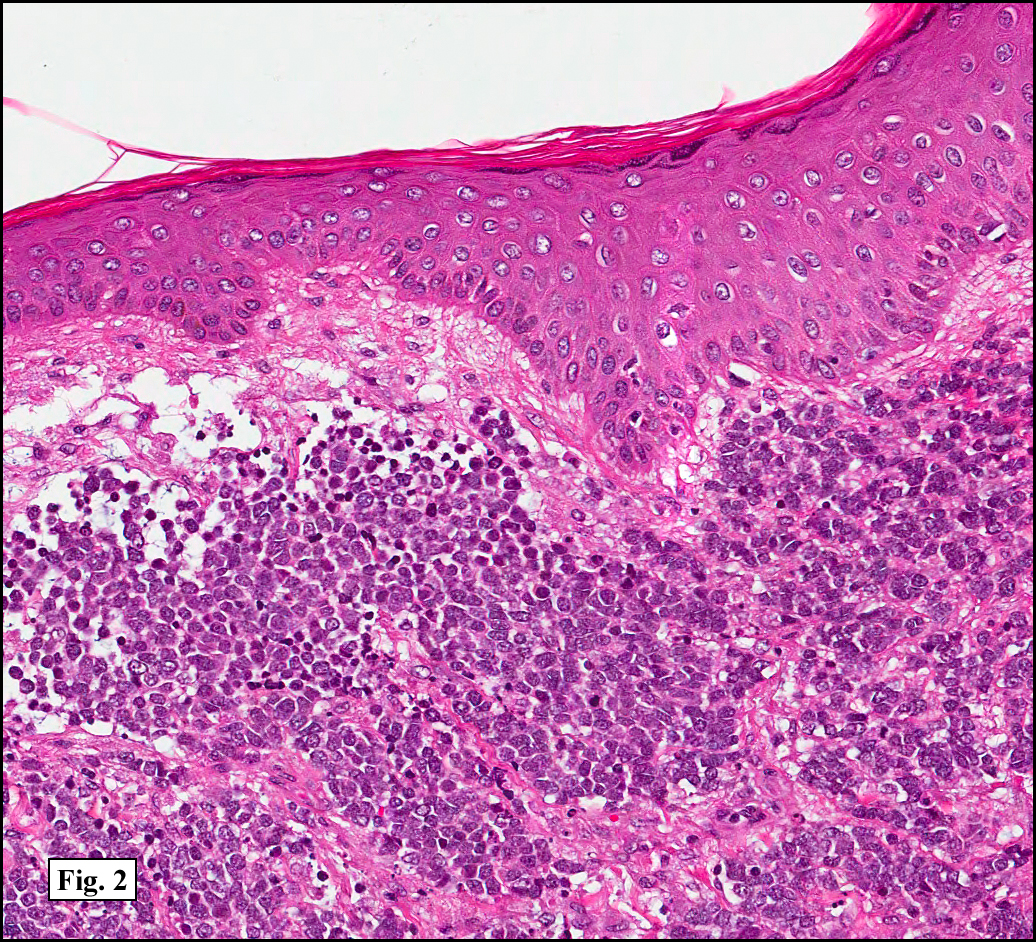
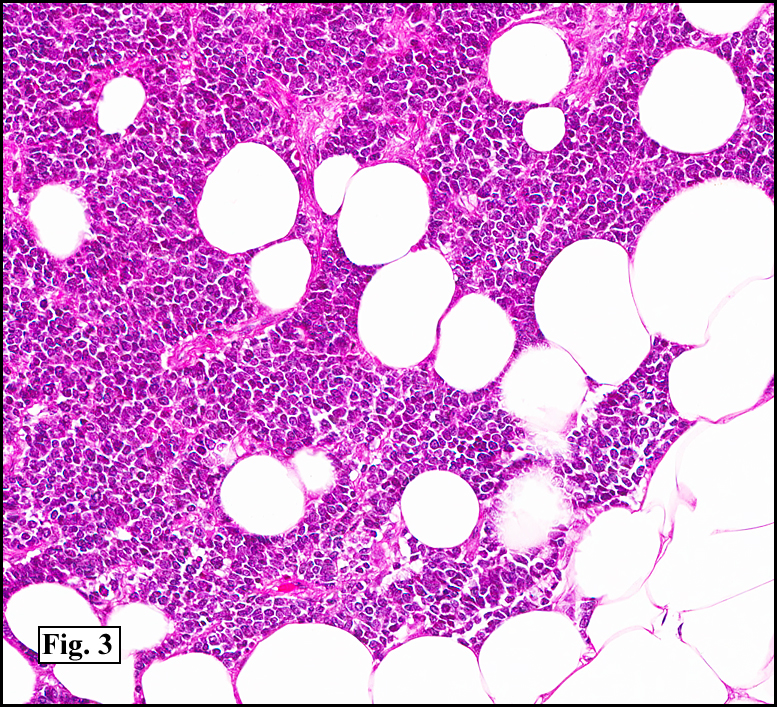
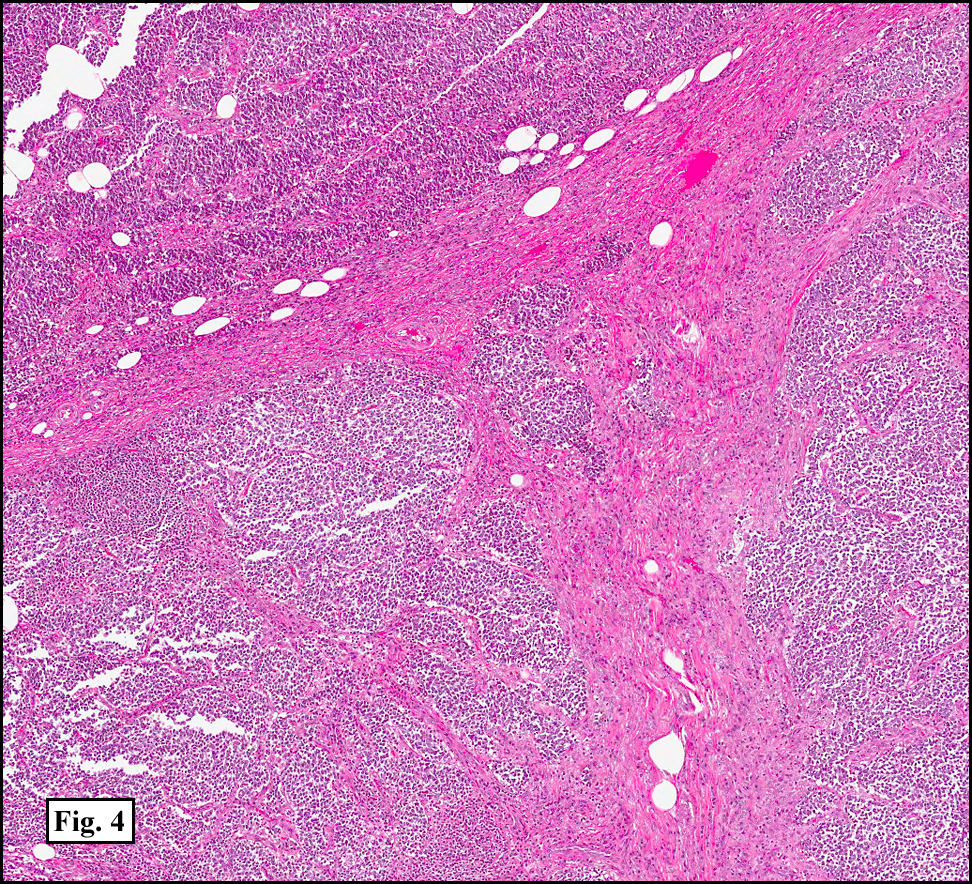
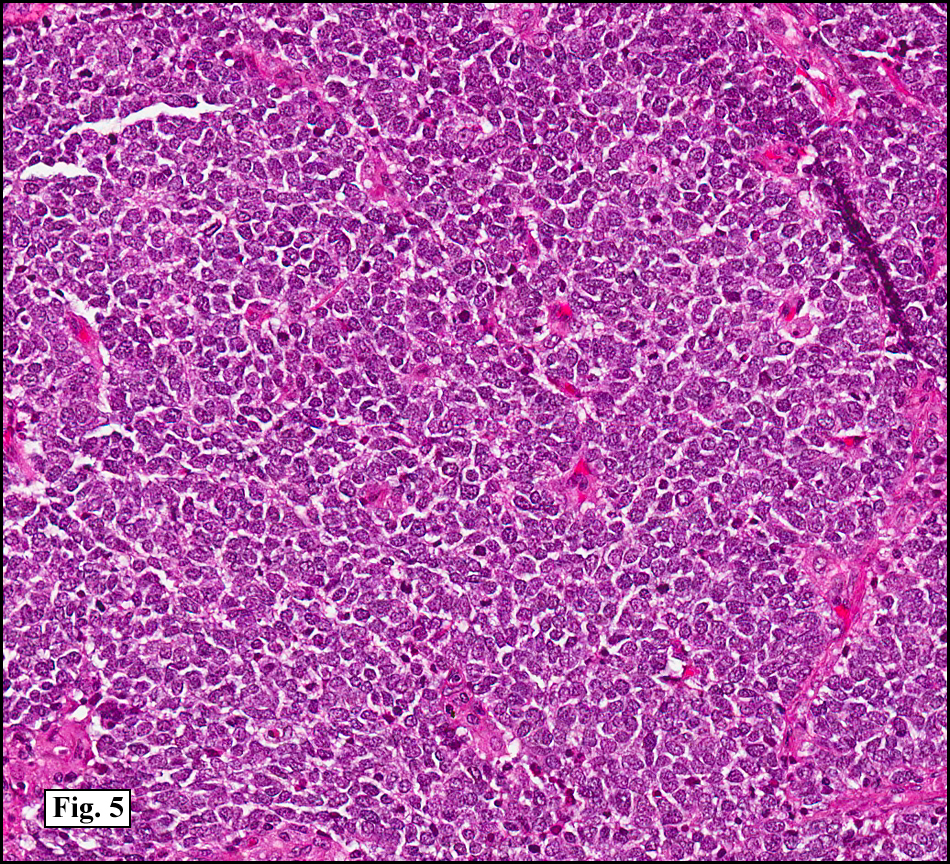
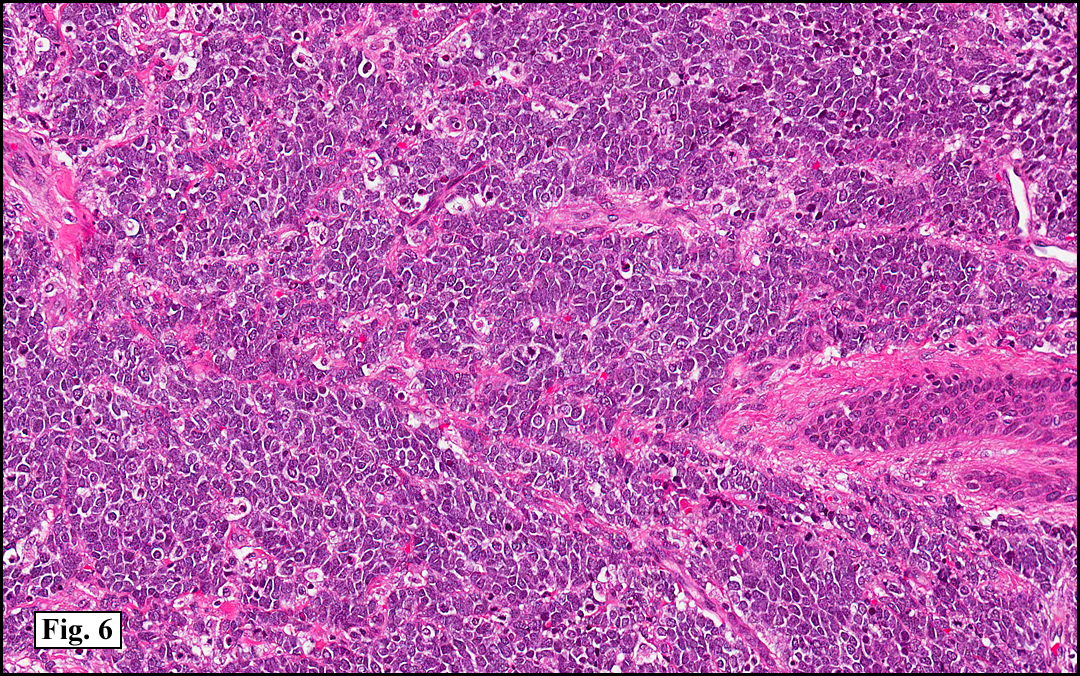
The biopsy showed a large, asymmetrical poorly-confined neoplasm (Fig. 1) extending from the papillary dermis (Fig. 2) into the subcutaneous fatty tissue (Fig. 3). The tumor showed a trabecular pattern with irregularly shaped tumor nodules between the stroma (Fig. 4). The closely packed neoplastic cells showed large, round vesiculated nuclei and inconspicuous nucleoli, aka “small round blue cells†(Fig. 5). Some regions showed hyper- and hypo-dense cell sheets. Scattered throughout the tumor were atypical mitotic figures and necrotic neoplastic cells (Fig. 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Merkel Cell Carcinoma, Buttockâ€
Jonathan Zumwalt, PSF, and Donald R. Chase, MD
Department of Pathology and Human Anatomy, Loma Linda University and
Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: First described about in 1972 by Toker as “trabecular carcinomaâ€, Merkel cell carcinoma was later ultrastructurely shown to have neuroendocrine granules identical to those found in Merkel cells of the epidermis, cells which share similar ultrastructure and biochemistry as the tumor first described by Toker and Friedrich Sigmund Merkel in 1875. They are neural crest derived cells usually located in the DEJ or within adnexal epithelium. They play roles as both mechanoreceptors and endocrine cells for the sensory system: light touch discrimination of shapes and textures.
Merkel cell carcinoma (MCC), an epithelial neuroendocrine cell tumor, is included in the APUD system (amine precursor uptake and decarboxylase system). It is believed that malignant transformation takes place in the cell of origin as a result of chronic exposure to ultraviolet radiation. Molecular alterations found in Merkel cell carcinoma include deletion of the short arm of chromosome 1, trisomy 6 and loss of heterozygosity of chromosome 13.
The clinical presentation of MCC is typically of a small growing firm nodule on the head or neck of patients with sun damage. The average size of the tumor is typically 2.0 cm. MCC can occasionally grow to tremendous proportions up to 20 cm. Checking for lymphadenopathy is critical for the clinician, due to there being metastasis to local nodes 30% at the time of diagnosis.
MCC is most commonly found in older Caucasian men with previous sun damage. The age range of MCC incidence is 40-90; with the most common group in ages 70-80. Fifty per cent of tumors are on the head and neck, 35% are on the extremities and 15% are on the chest, back and abdomen. There is an increased incidence of MCC in patients with HIV, B-cell neoplasms, CLL and HIV, due to the immunosuppression of these diseases.
MCC acts very aggressively, and wide local excision is the treatment of choice after simple excision. Wide local excision decreases locoregional relapse of tumor by 3 fold (89% to 27%) and increases 2-year survival by 3 fold (28% to 86%) as compared to simple excision. The tumor is radiosensitive, but tends to reoccur after treatment. Radiation alone is usually used for palliative care. 10-year survival rates range from 30-70% depending on staging.
One of the most recent finding with MCC is its origin. In 2008, Drs. Chang and Moore at the University of Pittsburgh found a virus associated with the tumor. The virus coined, Merkel Cell Polyomavirus, is found in 80% of MCC tumors. The virus is infects most healthy humans by age 15 and infection is asymptomatic. Testing of healthy human tissue shows occasional infection of the virus. The virus is under the papovaviridae family, which includes the HPV (warts), BK (upper respiratory infection) and JC (progressive multifocal leukoencephaolopathy) viruses. The virus is non-transmissible after integration into the host genome, due to the truncation of the DNA during integration and the virus is only monoclonal after integration. Some researchers are even looking into a vaccine.
MCC has shown to regress spontaneously. This unique phenomenon has been documented 22 times in the literature. It accounts for 1.5% of the reported MCC cases. It is thought that the immune system is able to identify and eliminate the MCC virus. Similar to the mechanism in which the body is able to spontaneously dispose of skin warts.
There are three histologic subtypes of Merkel cell carcinoma:
– Trabecular Pattern: composed of ribbons of uniform cells with nuclear molding.
– Intermediate type formed by nodules and sheets of basophilic cells that show pale vesicular nuclei containing a small nucleolus.
– Small cell type: with small “oat cells” usually displaying crush artifact.
MCC is unique to other neuroendocrine tumors due to its immunohistochemical profile. The tumor expresses both epithelial and neuroendocrine markers. The most unique marker is cytokeratin 20, which usually stains with a typical perinuclear “dot-like†pattern. High molecular cytokeratins such as CAM 5.2 are also commonly expressed.
The cells may also show a spindled appearance. There is usually an elevated mitotic rate. Also, necrotic cells may be scattered throughout the tumor. Lymphatic and vascular invasion are commonly present (30%) and must be investigated due to prognostic factors and staging.
Sometimes the tumor shows epidermotropism. Additional epidermal findings include actinic keratosis and/or squamous cell carcinoma in situ. Fully developed adjacent squamous cell or basal cell carcinomas have also been described.
Differential Diagnosis:
Basal Cell Carcinoma: Basal cell carcinoma (BCC) is the most common mimicker of MCC. BCC differs in that is shows retraction between the stroma and tumor. BCC nuclei are also hyperchromatic and tend to palisade around the periphery of nests.
Melanoma: The small cells of neuroendocrine carcinoma of the skin can be initially interpreted as lymphoid or nevoid melanoma, especially considering that MCC can present with epidermotropism. Immunohistochemistry will readily exclude a lymphoma or a melanoma from the differential diagnosis.
Small Cell Carcinoma of the Lung may appear almost identical to MCC due to it being a neuroendocrine tumor and the age groups of the patients. The tumor is characterized by poor circumscription, and the extremely smudged interface between cells as well as a tendency for the distortion of the cells during preparation to form elongated basophilic strings. Small cell carcinoma is positive for TTF1 and CK7 staining.
Ewing Sarcoma: Ewing sarcoma usually occurs in a younger population and is rare in an adult. Extraskeletal Ewing’s sarcoma has cells that are less closely packed and the neoplasm is often large and deep-seated. The tumor stains positively for CD99.
Thanks
A special thanks to Martin Mihm and his 120th CTTR Semi-Annual Pathology Slide Seminar Handout.
Suggested Reading:
Albores-Saavedra J, Batich K, Chable-Montero F, Sagy N, Schwartz AM, Henson DE. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: a population based study. J Cutan Pathol. 2009 Jul 21.
Andea AA, Coit DG, Amin B, Busam KJ. Merkel cell carcinoma: histologic features and prognosis. Cancer. 2008 Nov 1;113(9):2549-58.
Bichakjian CK, Coit DG, Wong SL. Radiation versus resection for Merkel cell carcinoma. Cancer. 2010 Apr 1;116(7):1620-2.
Calder KB, Smoller BR. New insights into merkel cell carcinoma. Adv Anat Pathol. 2010 May;17(3):155-61.
Craig PJ, Calonje JE, Harries M, Stefanato CM. Incidental chronic lymphocytic leukaemia in a biopsy of Merkel cell carcinoma. J Cutan Pathol. 2009 Jun;36(6):706-10.
Ciudad C, Avilés JA, Alfageme F, Lecona M, Suárez R, Lázaro P. Spontaneous regression in merkel cell carcinoma: report of two cases with a description of dermoscopic features and review of the literature. Dermatol Surg. 2010 May;36(5):687-93. Epub 2010 Apr 1.
D’Agostino M, Cinelli C, Willard R, Hofmann J, Jellinek N, Robinson-Bostom L. Epidermotropic Merkel cell carcinoma: a case series with histopathologic examination. J m Acad Dermatol. 2010 Mar;62(3):463-8.
Duncavage EJ, Le BM, Wang D, Pfeifer JD. Merkel cell polyomavirus: a specific marker for Merkel cell carcinoma in histologically similar tumors. Am J Surg Pathol. 2009 Dec;33(12):1771-7.
Foulongne V, Dereure O, Kluger N, Molès JP, Guillot B, Segondy M. Merkel cell polyomavirus DNA detection in lesional and nonlesional skin from patients with Merkel cell carcinoma or other skin diseases. Br J Dermatol. 2010 Jan;162(1):59-63. Epub 2009 Jul 6.
Heath M, Jaimes N, Lemos B, Mostaghimi A, Wang LC, Peñas PF, Nghiem P. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008 Mar;58(3):375-81.
Heymann WR. Merkel cell carcinoma: insights into pathogenesis. J Am Acad Dermatol. 2008 Sep;59(3):503-4.