 History: A 66 year old male presented with increasing left upper quadrant abdominal pain of two weeks duration. Physical examination showed splenomegaly and multiple violaceous, indurated, non-erythematous cutaneous nodules on the back and torso that ranged from 3 to 6 cm in diameter.
History: A 66 year old male presented with increasing left upper quadrant abdominal pain of two weeks duration. Physical examination showed splenomegaly and multiple violaceous, indurated, non-erythematous cutaneous nodules on the back and torso that ranged from 3 to 6 cm in diameter.
A CT scan showed splenomegaly and mild abdominal lymphadenopathy as well as scattered small lymph nodes in the pretracheal region, suspicious for lymphoma.
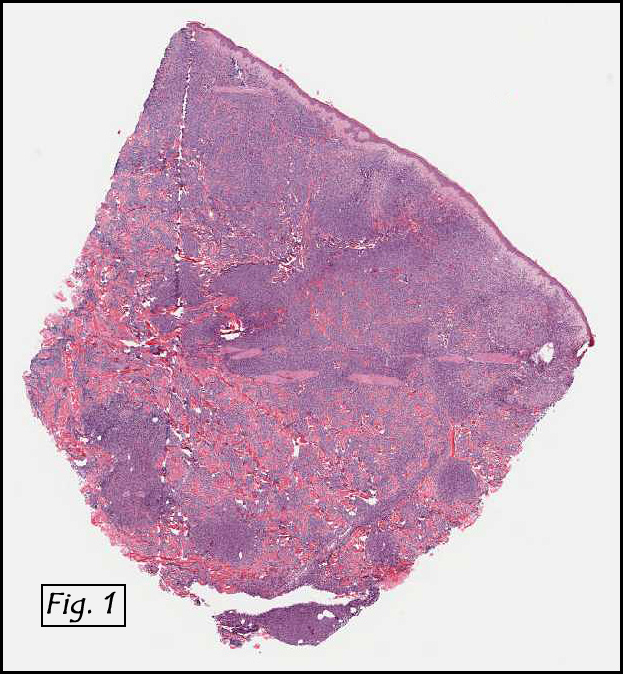
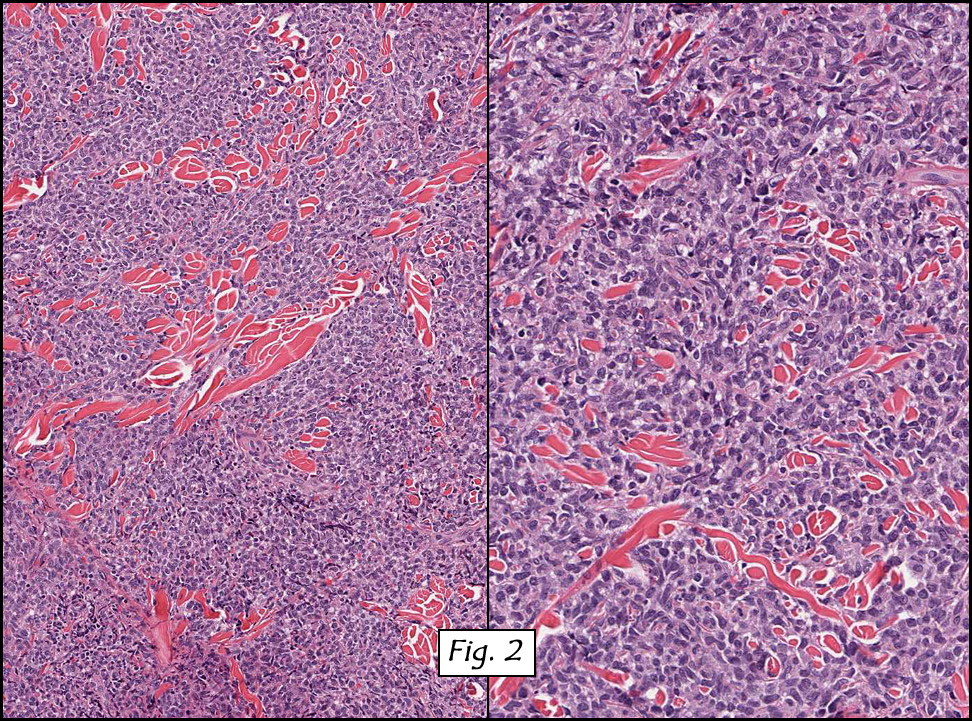
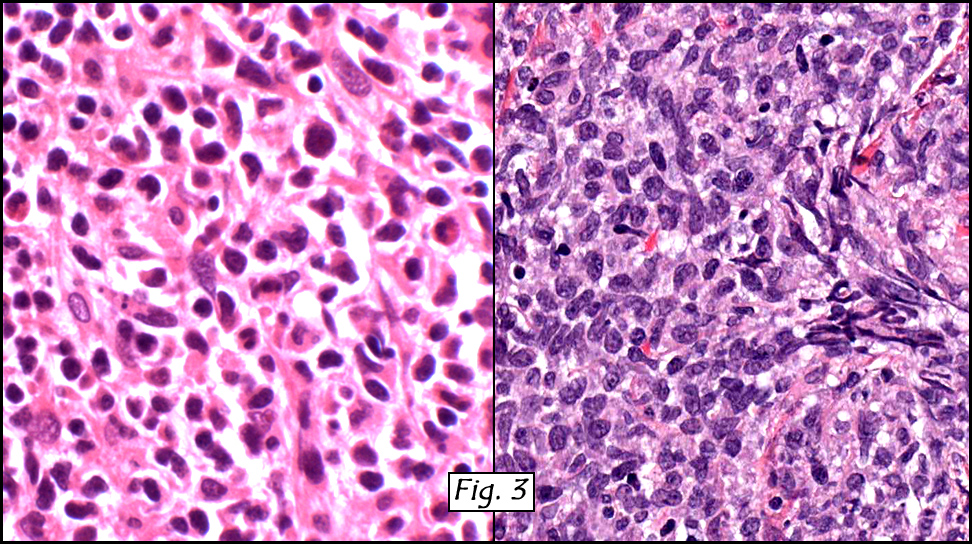
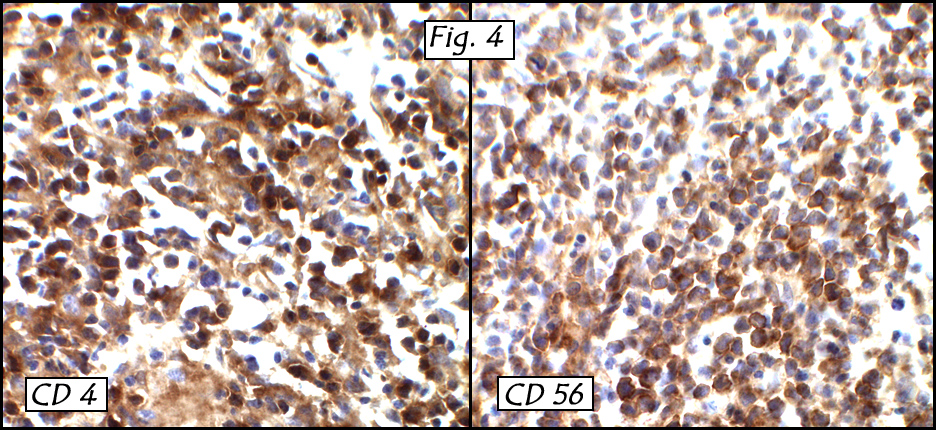
A skin biopsy showed a dense atypical monomorphic cell infiltrate involving the full thickness of the dermis with extension into the subcutis (Fig. 1). The cells were medium to large in size with oval or folded nuclei, smooth to granular chromatin, occasional nucleoli, and small to moderate amount of pale eosinophilic cytoplasm (Fig. 2-3). Mitotic figures and scattered apoptotic bodies were common. The overlying epidermis was unremarkable and there was a well preserved Grenz zone. The tumor cells were positive for CD4 and CD56 (Fig. 4) as well as for CD43 and focally weakly for CD163. They were negative for CD3, CD20, CD79a, myeloperoxidase, cytotoxic T-cell marker TIA-1, Granzyme-B and CD57.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The patient also had pancytopenia with about 6% atypical mononuclear cells in the peripheral blood. The marrow biopsy was solidly cellular and the aspirate yielded a dry tap. The bilateral trephine biopsies showed 50% infiltration by tumor cells which were similar to those seen in the skin biopsy. The tumor cells stained positively for CD4 and CD56. Immunophenotyping by flow cytometry showed 25% of the neoplastic cells expressing CD4 dim, CD5, CD38, CD43, CD45, CD56, and HLA-DR, but not CD2, cytoplasmic or surface CD3, CD7, CD8, TdT, and/or other myeloid and monocytic markers.
Diagnosis: “CD4+/CD56+ Hematodermic Neoplasmâ€
Renuka Agrawal M.D., Jun Wang M.D., and Donald R. Chase M.D.
Department of Pathology, Loma Linda University and Medical Center
California Tumor Tissue Registry
Discussion: Hematodermic neoplasm is the favored term for a neoplasm formerly known as blastic NK-cell lymphoma which is CD4 and CD56 positive (per the WHO and the European Organization for the Research and Treatment of Cancer (EORTC) consensus classification for cutaneous lymphomas). It was first described by Adachi et al in 1994.
Hematodermic Neoplasm (HDN) is a rare malignancy, which typically affects middle aged or elderly patients, usually males, who initially present with widespread skin infiltration (purplish papules, nodules, or bruise like skin lesions), that have a predilection for the trunk but may also involve the extremities and the head and neck, followed closely by lymph node, spleen and bone marrow involvement, often terminating in the leukemic phase with a fatal course.
Histologically, these tumors involve the dermis and sometimes the subcutaneous tissue, but show no epidermotropism. The infiltrates are composed of monotonous, medium sized mononuclear cells, with sparse cytoplasm and finely dispersed chromatin, and absent or indistinct nucleoli resembling lymphoblasts or myeloblasts. Frequent mitotic figures may be seen, but there is generally no necrosis or angioinvasion.
The cell of origin is believed to be a plasmacytoid dendritic cell precursor which appears to be related to plasmacytoid monocytes because it also expresses CD68 and bright levels of CD123. High levels of CD123 (IL3 receptor alpha chain) is a distinctive characteristic of plasmacytoid monocytes and HDN and can probably be used for either prognostic or therapeutic purposes as well as CD20 in B-cell lymphomas.
The tumor cells usually have a staining pattern of CD4+, CD56+, CD8-, CD7-/+,
CD2-/+, CD43+, CD45RA+, and do not express surface and cytoplasmic CD3 nor cytotoxic proteins. TdT may be positive.
As lymphoblastic and myeloblastic neoplasms can also be positive for CD56, stains for CD3 and myeloperoxidase should always be performed to exclude them. Rarely, myelomonocytic cells co-express CD4, CD56, and CD123. Therefore, high levels of CD123 expression can be used to discriminate HDN from non-Hodgkin’s lymphoma but alone are not sufficient to rule out myelomonocytic malignancies.
T-cell receptor genes are not rearranged and there is no association with oncogenic transformation by Epstein Barr virus.
HDN has a highly aggressive behavior and poor prognosis with a median survival time of 14 months. Patients are best treated with regimes used in acute leukemias. Although chemotherapy usually results in complete remission there is almost always a quick relapse unresponsive to further chemotherapy.
Suggested Reading:
1. Jean Feuillard et al. Clinical and Biologic Features of CD4+ CD56+ Malignancies. Blood, 1 March 2002; 99 (5):1556-1563
2. Patrella T, Comeau MR, Maynadie M et al. Agranular CD4+ CD56+ Hematodermic Neoplasm (Blastic NK-cell Lymphoma) Originates from a Population of CD56+ Precursor Cells Related to Plasmacytoid Monocytes. Am J.Surg Pathol. 2002; 26:852-862.
3. Willemze R. Jaffe ES, Burg G et al. WHO-EORTC Classification for Cutaneous Lymphomas. Blood. 2005; 105: 3768-3785.
4. J M Martin et al. CD4+CD56+ Hematodermic Neoplasm: A Precursor Hematological Neoplasm that Frequently First Presents in the Skin. JEADV 2006, 20; 1129-1132.
5. Urosevic M et al. CD4+CD56+ Hematodermic Neoplasms Bear a Plasmacytoid Dendritic Cell Phenotype. Hum Pathol. 2005; 36:1020-1024.
6. Niakosari F, Sur M. Agranular CD4+/CD56+ Hematodermic Neoplasm. Arch pathol Lab Med. January 2007; 131:149-151.
7. Adachi M, Maeda K, Takekawa M, et al. High expression of CD56 (N182CAM) in a patient with cutaneous CD4-positive lymphoma. Am J Hematol. 1994; 47: 278-282.
8. Ng AP; Lade S; Rutherford T; McCormack C; Prince HM; Westerman DA. Primary cutaneous CD4+/CD56+ hematodermic neoplasm (blastic NK-cell lymphoma): a report of five cases. Haematologica 2006 Jan;91(1): p143-4.
9. Wu HH; Ren R; Roepke JE. Fine-needle aspiration cytology of blastic natural killer-cell lymphoma (CD4+ CD56+ hematodermic neoplasm). Diagn Cytopathol 2004 Apr;30(4): p268-70.
10. Petrella T; Bagot M; Willemze R; Beylot-Barry M; Vergier B; Delaunay M; Meijer CJ; Courville P; Joly P; Grange F; De Muret A; Machet L; Dompmartin A; Bosq J; Durlach A; Bernard P; Dalac S; Dechelotte P; D’Incan M; Wechsler J; Teitell MA. Blastic NK-cell lymphomas (agranular CD4+CD56+ hematodermic neoplasms): a review. Am J Clin Pathol 2005 May;123(5): p662-75.