 History: A 48 y/o woman underwent a hysterectomy and right salpingo-oophorectomy ten years previously for an enlarged uterus. A large number of blood vessels were found throughout the endometrium and myometrium that were commented upon as being “unusual/uncertainâ€. Ten years later she presented with microscopic hematuria and severe pain radiating to her back. An IVP identified a pelvic mass which was biopsied and later excised. Following removal of the mass the CA-125, which had been elevated, returned to normal limits.
History: A 48 y/o woman underwent a hysterectomy and right salpingo-oophorectomy ten years previously for an enlarged uterus. A large number of blood vessels were found throughout the endometrium and myometrium that were commented upon as being “unusual/uncertainâ€. Ten years later she presented with microscopic hematuria and severe pain radiating to her back. An IVP identified a pelvic mass which was biopsied and later excised. Following removal of the mass the CA-125, which had been elevated, returned to normal limits.
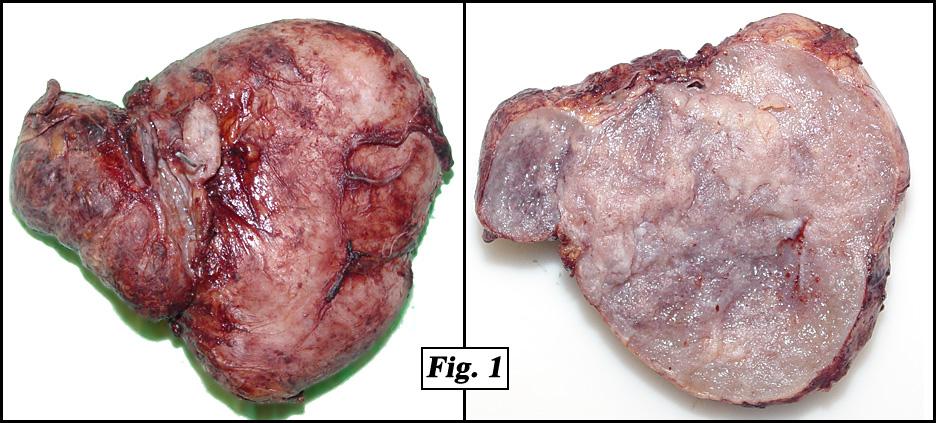
The removed pyriform mass was 9.3 x 8.6 x 3.9 cm and well-circumscribed, weighing 164 grams. The cut surface was solid and grey to focally flesh-colored (Fig. 1).
{kind=link}
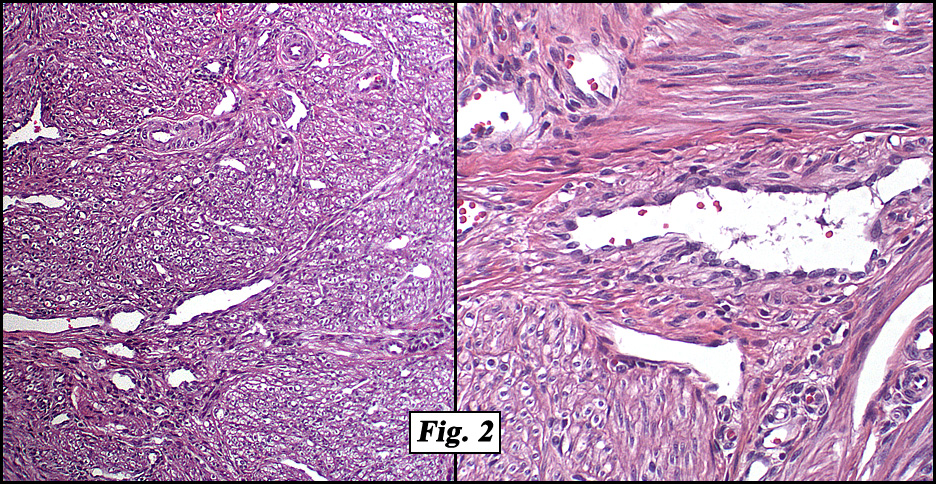
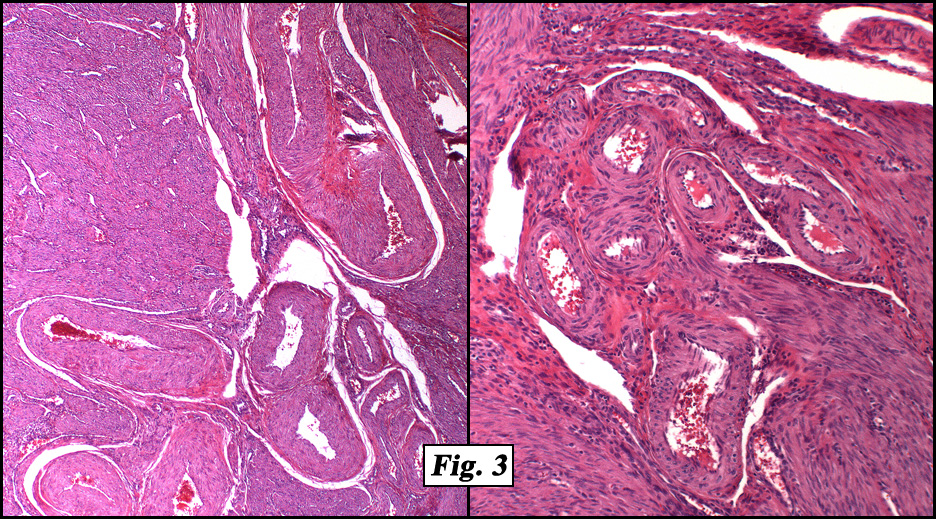
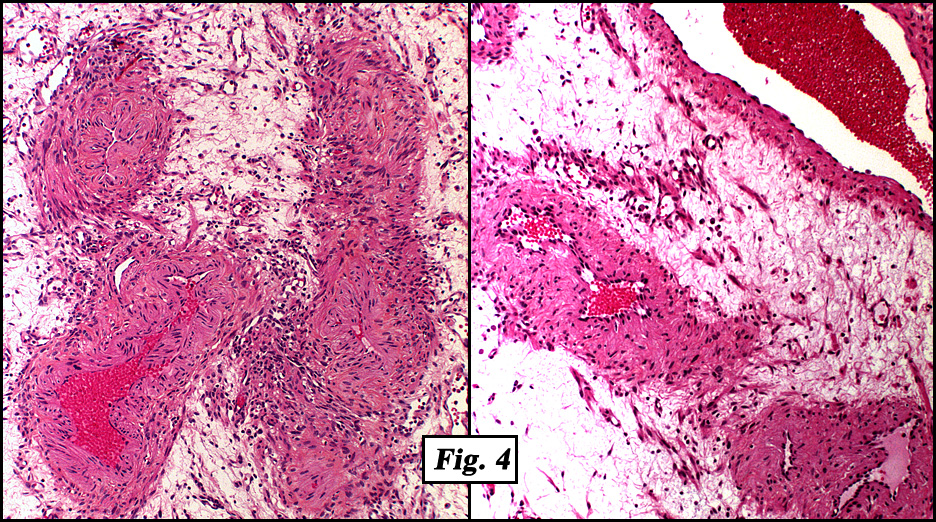
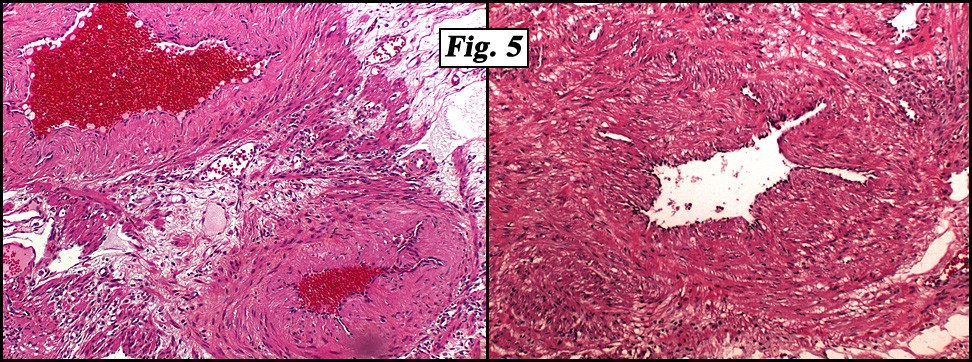
Microscopically, the tumor was well-delineated but not encapsulated. There were numerous small to intermediate-sized blood vessels generally with muscular investiture surrounded by additional myogenous tissue which appeared to “peel†off the outer walls extending outward into the rest of the neoplasm (Fig. 2,3). Other areas showed bends of smooth muscle cells in a very edematous tissue (Figs. 4, 5). All muscular components were uniform without significant pleomorphism or mitotic figures. There were also a small number of eosinophilic leukocytes and mast cells.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Angioleiomyoma (Uterine and Pelvic)â€
Wafaa Elatre, MD, Fouad Abdelhalim, MD, Donald R. Chase MD
Department of Pathology and Human Anatomy,
Loma Linda University and Medical Center, Loma Linda, CA
California Tumor Tissue Registry, Loma Linda, CA
Discussion: Angioleiomyoma is a benign neoplasm that may be small or large, huge, and/or multiple. It is composed of thick-walled vessels and smooth muscle cells. It usually develops between the fourth and sixth decades and when small is usually painless especially when it is located in the head and neck region. However, pain is the dominant clinical feature of uterine angioleiomyoma. The mechanism of pain is inconclusive but may be attributable to local ischemia from vessel contraction. Bleeding is common and uterine angioleiomyoma can cause severe menorrhagia. It is speculated that the abnormal bleeding may be due to local dysregulation of the vascular structures in the uterus or due to secretion of various growth factors.
Grossly, angioleiomyoma presents as circumscribed gray-white nodule or nodules. It can have dilated vessels mistaken for a multiloculated/multiseptated ovarian tumor or even for adenomyosis
Microscopically, angioleiomyoma is usually well-demarcated, composed of whorled, anastomosing fascicles of uniform, fusiform smooth muscle cells with thick-walled vessels. Areas of myxoid change, hyalinization, calcification, and fat may be seen. Mitotic figures and necrosis are infrequent.
Angioleiomyomas are classified into three histological types:
• solid
• capillary or cavernous, and
• venous
The nature of the vessels is controversial. Some authors have suggested that they are derived from arteriovenous anastomoses.
If the vascular component predominates it may be difficult to distinguish an angioleiomyoma from a hemangioma or an arteriovenous malformation. However, angioleiomyomas are always well-circumscribed and have foci of typical spindled smooth muscle cells. Uterine hemangiomas are exceptionally rare and unlike angioleiomyoma are poorly defined both grossly and microscopically.
Surgical excision is the treatment of choice. Either angiomyomectomy or simple hysterectomy for women who do not wish to have more children have proved to be effective treatments.
In conclusion, uterine angioleiomyoma should be considered when prominent tortuous vascular-like enhancing structures are noted on CT examination of a well-demarcated soft tissue mass arising from the uterus in pelvis. Either angiomyomectomy with tumor-free margins or hysterectomy have proven to be effective treatments and have resulted in satisfactory outcomes.
Suggested Reading:
- Weiss SW, Goldblum JR. Benign tumors of smooth muscle. In: Enzinger and Weiss’s Soft Tissue Tumors. 4th ed., Mosby, St. Louis, pp 699-700, 2001.
- Zaloudek C, Hendrickson MR: Mesenchymal tumors of the uterus. In: Blaustein’s Pathology of the Female Genital Tract. (Ed.: Kurman R), 5th ed, Springer-Verlag, New York, pp 574, 2002.
- Hennig Y, Caselitz J, Stern C, et al: Karyotype evolution in a case of uterine angioleiomyoma. Cancer Genet Cytogenet 108:79-80, 1999.
- Wang CP, Chang YL, Sheen TS: Vascular leiomyoma of the head and neck. Laryngoscope 114: 661-665, 2004.
- Ide F, Mishima K, Saito I: Angiomyoma in the submandibular gland: a rare location for an ubiquitous tumour. J Laryngol Oto l117:1001-1002, 2003.
- Hsieh CH, Lui CC, Huang SC, et al: Multiple uterine angioleiomyomas in a woman presenting with severe menorrhagia. Gynecol Oncol 90: 348-352, 2003.
- Stewart EA, Nowak RA: Leiomyoma-related bleeding: a classic hypothesis updated for the molecular era. Hum Reprod Update 2:295-306, 1996.
- Agorastos T, Dinas K, Patsiaoura K: Cystic degenerated angioleiomyoma mimicking ovarian pathology. Acta Obstet Gynecol Scand 80:863-865, 2001.
- Nil C, Esra O, Hasan Y, Yelda O Emel U. Spontaneously Ruptured Uterine Angioleiomyoma Pathology Oncology Research Vol 12, No 1, 50–51