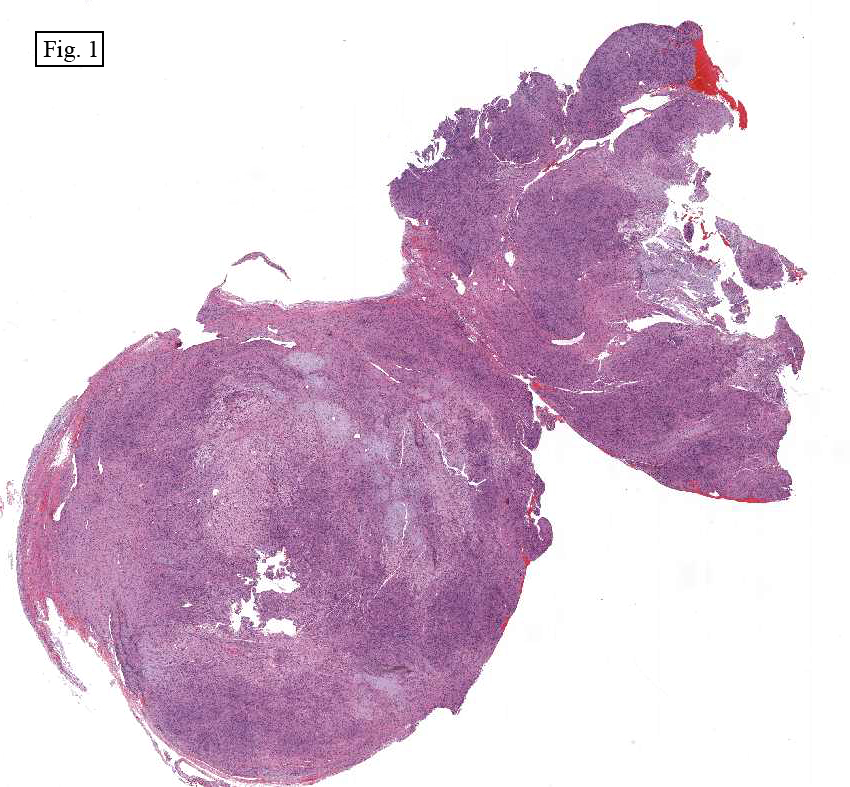
History: A 44 year old man with a seven year history of persistent right nasal congestion and right facial paresthesia was found to have a mass in the right maxillary sinus. A CT scan demonstrated a 4.0 x 3.8 x 3.2 cm well-circumscribed lesion with focal cystic change and palatine extension. The excised specimen consisted of a 23 gm aggregate of firm, variegated yellow and white hemorrhagic soft tissue fragments.
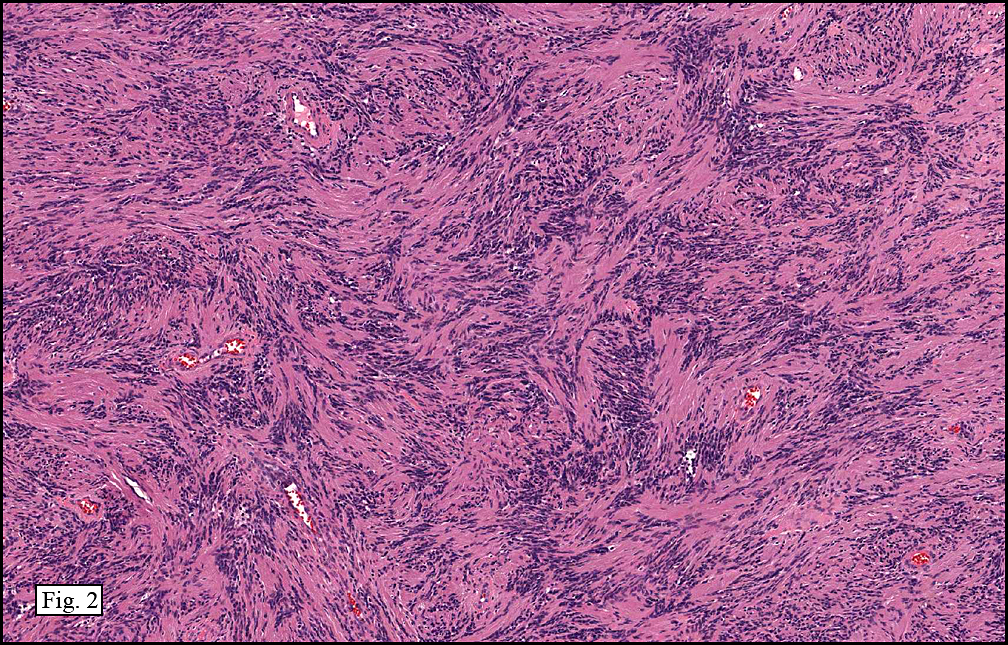
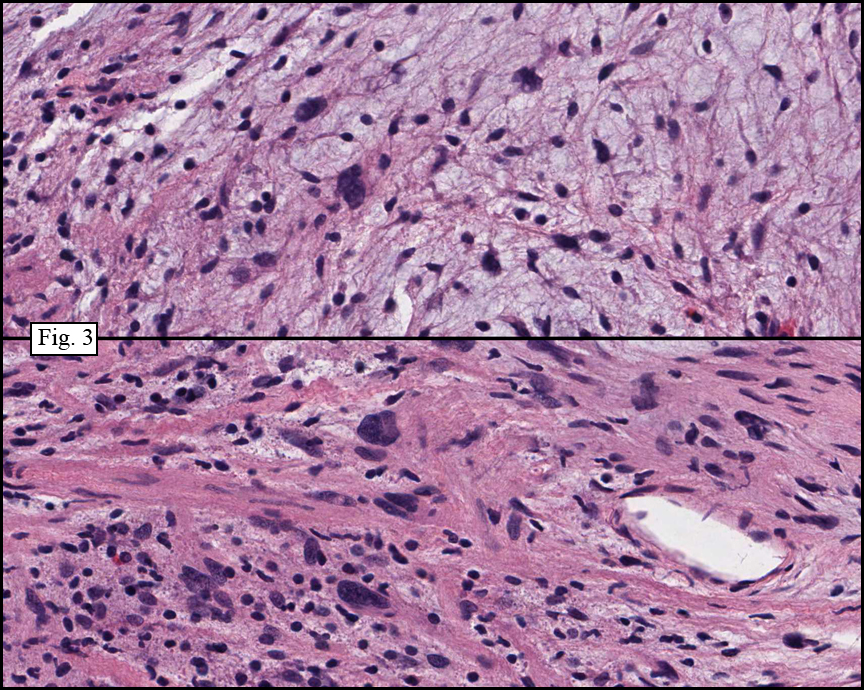
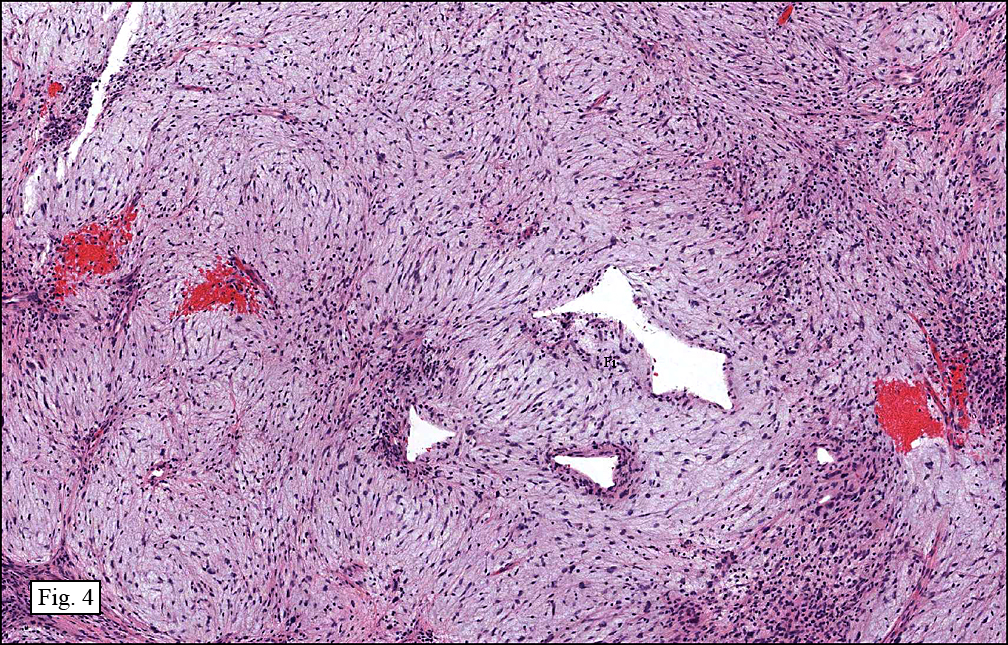
Microscopically, the tumor consisted of spindle cells with wavy nuclei in cellular and hypocellular regions (Fig. 1). The cellular regions contained short fascicles with nuclear palisading (Fig. 2). Frequently seen were mildly enlarged hyperchromatic atypical nuclei, however; mitoses were not identified (Fig. 3). The hypocellular areas were less ordered and had a loose matrix (Fig. 4). Also present were foamy histiocytes, hyalinized vessels, cyst-like spaces, a mixed inflammatory infiltrate and hemorrhage as well as increased fibrous tissue (Fig. 5). Necrosis was not seen.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Schwannoma with Degenerative Change/Ancient Schwannomaâ€, Maxillary Sinus
Adam Stelling, PSF, MS3, Donald R. Chase MD
Department of Pathology and Human Anatomy, Loma Linda University and Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Ancient schwannoma is a rare benign peripheral nerve sheath tumor felt to derive from a long standing schwannoma. The lesion occurs most commonly in patients between 20 and 50 years of age. The classic schwannoma is an encapsulated perineural mass consisting of highly cellular Antoni A areas with Verocay bodies and less cellular myxoid Antoni B areas. They are most often found in the head and neck, flexor surfaces of the extremities, paraspinal areas as well as the retroperitoneum. Schwannomas make up approximately 8% of intracranial tumors with the vestibulocochlear nerve most commonly involved followed by the trigeminal and facial cranial nerves. Tumors with “ancient change†demonstrate the same behavior as a classic schwannoma and tend not to recur following excision.
The degenerative component of an ancient schwannoma creates a heterogeneous gross appearance with calcification and cystic change within a firm grey, yellow and tan cut surface. Beware that sinonasal schwannomas are often unencapsulated. Microscopically, large irregular hyperchromatic nuclei are a hallmark feature and should not be confused with malignancy. Absent mitotic figures and an appropriate histologic background make this finding most consistent with degenerative atypia. Other common features include histiocytic infiltrates with xanthomatous change and hyalinized vascular walls. Varying amounts of non-specific degenerative changes such as edema, myxoid change, hemorrhage, inflammation and fibrosis are seen.
The single most influential tool in differentiating ancient schwannoma from its mimics is the highly sensitive expression of S-100 protein. Uniform strong positive staining in both Antoni A and B areas supports the notion that the tumor is made up of a single population of neoplastic Schwann cells: a hypothesis confirmed by ultrastructural EM studies.
Differential diagnoses:
Neurofibroma – This unencapsulated benign peripheral nerve sheath tumor has wavy spindled nuclei in a background of prominent collagen in a “shredded carrot†pattern. Prominent cellular or myxoid areas may be present. Wagner-Meissner bodies are a classic feature, particularly in diffuse forms. S-100 positivity is only seen in a subset of cells thought to be of schwannian origin. Typically, neurofibromas do not contain degenerative changes, however; malignant change, more commonly seen in patients with neurofibromatosis type 1, manifests as nuclear atypia.
MPNST – The malignant peripheral nerve sheath tumor has alternating cellular and myxoid areas creating a so called “marble-like†pattern. This lesion contains wavy spindle cells that can palisade, as well as exhibit pleomorphism. Key distinguishing features include necrosis, mitoses, heterologous elements and only weak focal S-100 reactivity in spindled areas. Look for invasion, especially perineural, to confirm malignancy.
Leiomyosarcoma – In contrast to peripheral nerve tumors, smooth muscle tumors tend to have blunt ended “cigar-shaped†spindle nuclei. A fascicular growth pattern and focal hyalinization as well as nuclear palisading and pleomorphism are common, but S-100 is negative. Desmin, calponin and smooth muscle actin are typically positive. Leiomyosarcomas commonly demonstrate increased mitotic activity and necrosis.
Myxoid MFH – The prominent myxoid appearance in this lesion may resemble Antoni B regions of an ancient schwannoma. Other areas that still resemble the classic spindled storiform MFH may palisade yet should not have wavy nuclei. S-100 is negative in this tumor.
Calcifying aponeurotic fibroma – This lesion typically presents in the hands and feet of children and adolescents. This tumor contains palisading spindle cells as well as calcification or cartilage formation. The age of the patient, location of the tumor and S-100 negativity can aid in excluding this differential.
Suggested Reading:
Bruner, J. M. “Peripheral Nerve Sheath Tumors of the Head and Neck.” Semin Diagn Pathol. 4.2 (1987): 136-49. PubMed. Web. 13 May 2010.
Dodd, L. G., E. M. Marom, R. C. Dash, M. R. Matthews, and R. E. McLendon. “Fine-needle Aspiration Cytology of “ancient” Schwannoma.” Diagn Cytopathol. 20.5 (1999): 307-11. PubMed. Web. 13 May 2010.
Fletcher, C. D. “Distinctive Soft Tissue Tumors of the Head and Neck.” Mod Pathol 15.3 (2002): 324-30. www.nature.com/modpathol Web. 13 May 2010.
Hennigan, T. W., A. C. Branfoot, and N. A. Theodorou. “Ancient Neurilemmoma of the Pelvis.” J R Soc Med 85.7 (1992): 416-17. PubMed. Web. 17 May 2010.
Weiss, S. W., J. M. Langloss, and F. M. Enzinger. “Value of S-100 Protein in the Diagnosis of Soft Tissue Tumors with Particular Reference to Benign and Malignant Schwann Cell Tumors.” Lab Invest. 49.3 (1983): 299-308. PubMed. Web. 12 May 2010.
Weiss, Sharon W., John R. Goldblum, and Franz M. Enzinger. Enzinger and Weiss’s Soft Tissue Tumors. Philadelphia, PA: Mosby Elsevier, 5th ed. 2008.
Wed, Jul 27, 2011
This case would be paradigmatic in the context of cranial nerves schwannomas ( inscribed or not in clinical vestibular schwannomatosis ) .The typical description of Leu YS and Chang KC , overviewed the patient pool with cranial schwannomas ( Leu YS .Extracranial head and neck schwannomas : A review of 8 years experience .Acta Otolaryng 2002 ; 122: 435 ) or the series by Sarma S ; Sekhar LN and Schessel DA. Non vestibular schwannomas of the brain : A 7-year experience.Neurosurgery 2002 ; 50 : 437.Or the specific description in Neurosurgery 2002; 96: 453 . of trigeminal schwannomas ( dumbell-shaped tumours through the expanded Meckel cavum and outcomes of cranial nerve function.AlMefty et al.Or the series of a third of the primary V cranial nerve and the frequency of neuromas of the third , fourth and sixth cranial nervas ( Celli P Surg Neurol 1992 )
Considering d.d. of international consensus on MPNS tumour ( Cancer Res 2002 ) would be illustrative in this cases and valuable in this case.
Dr Sabino Guillermo Echebarria Mendieta
neurologist
Hospital San Eloy ( Barakaldo-Bizkaia ) district clinics.
Osakidetza-Basque Health Service