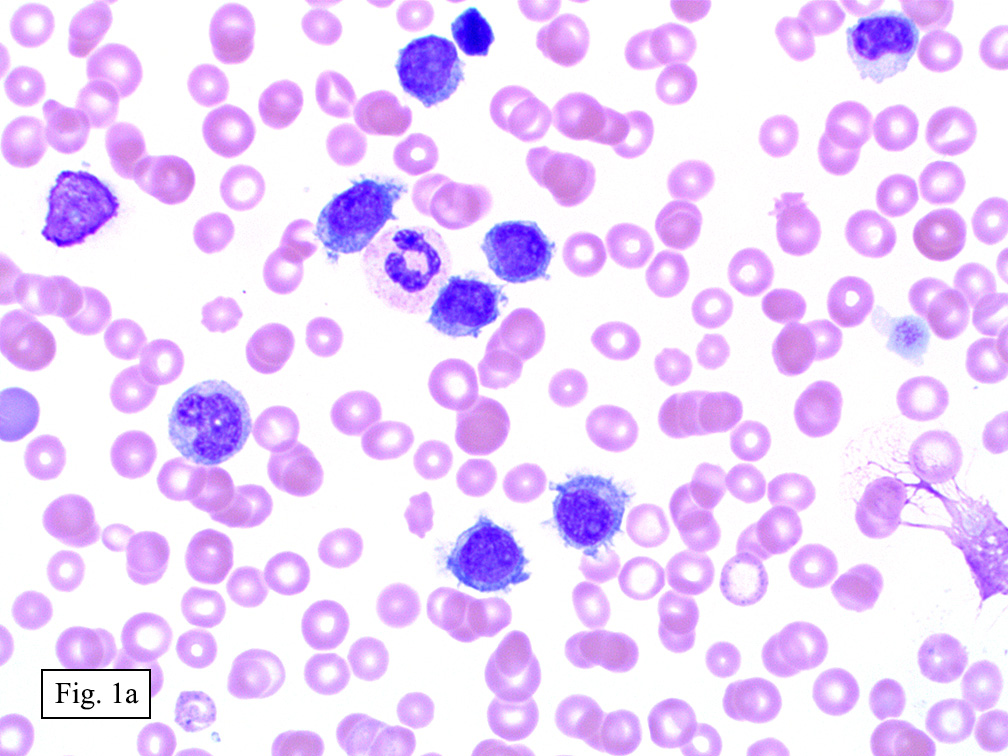
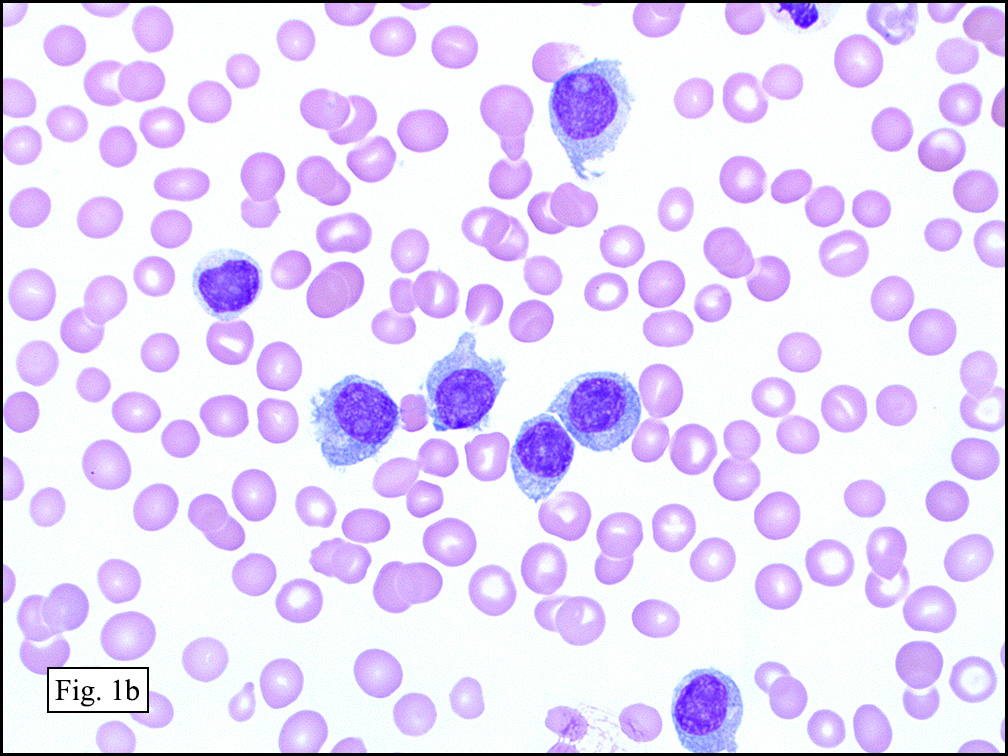
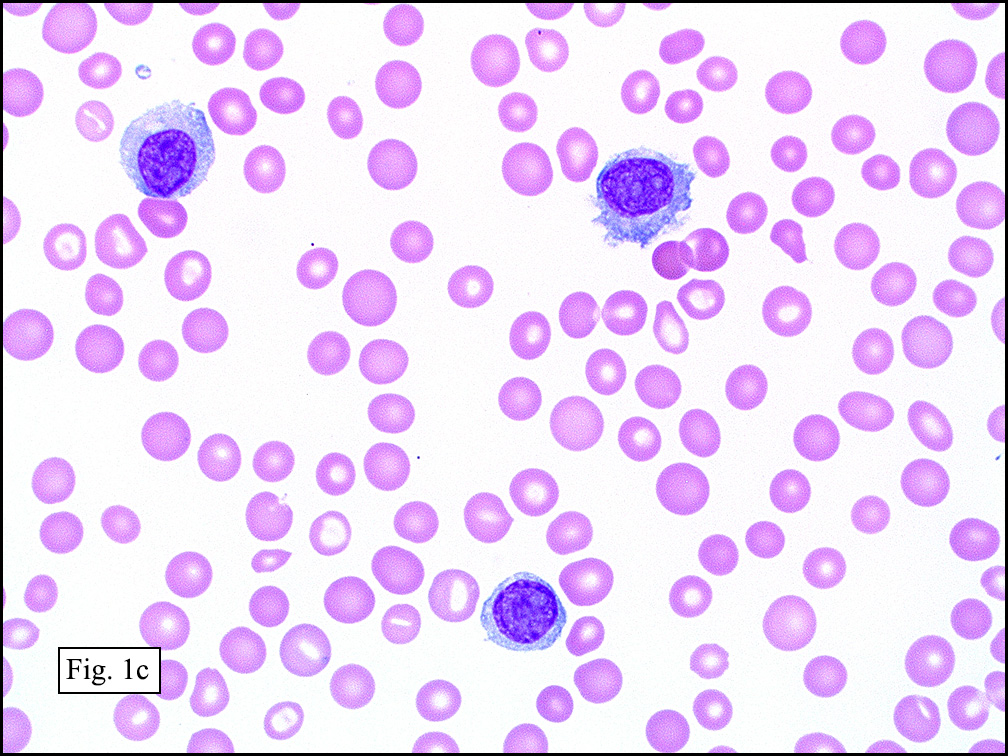
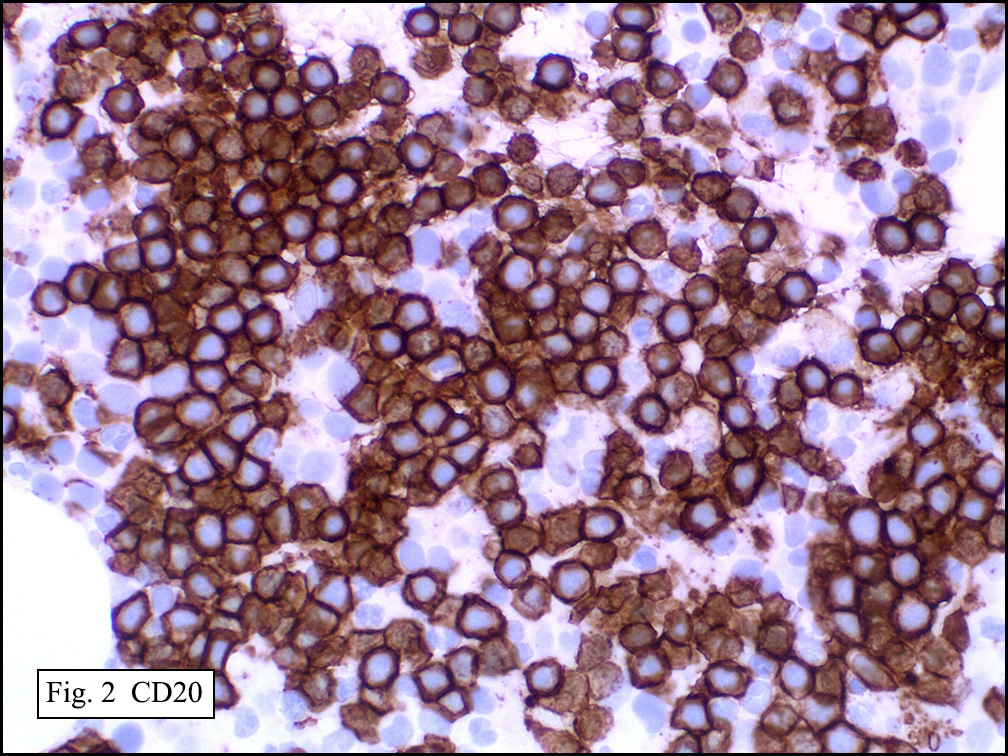
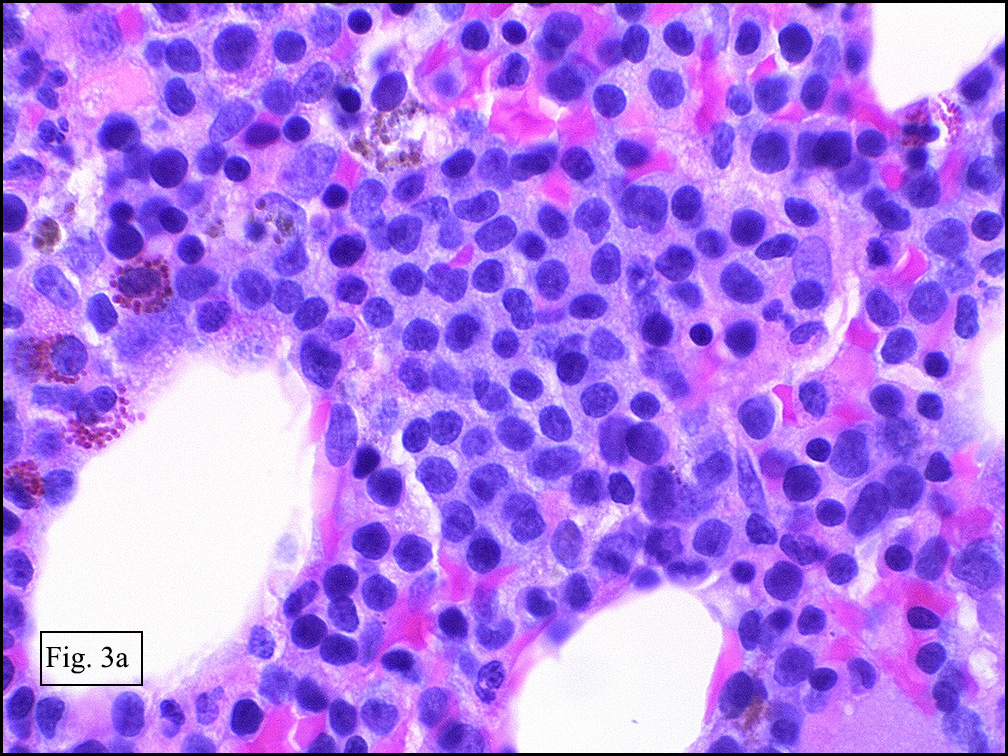
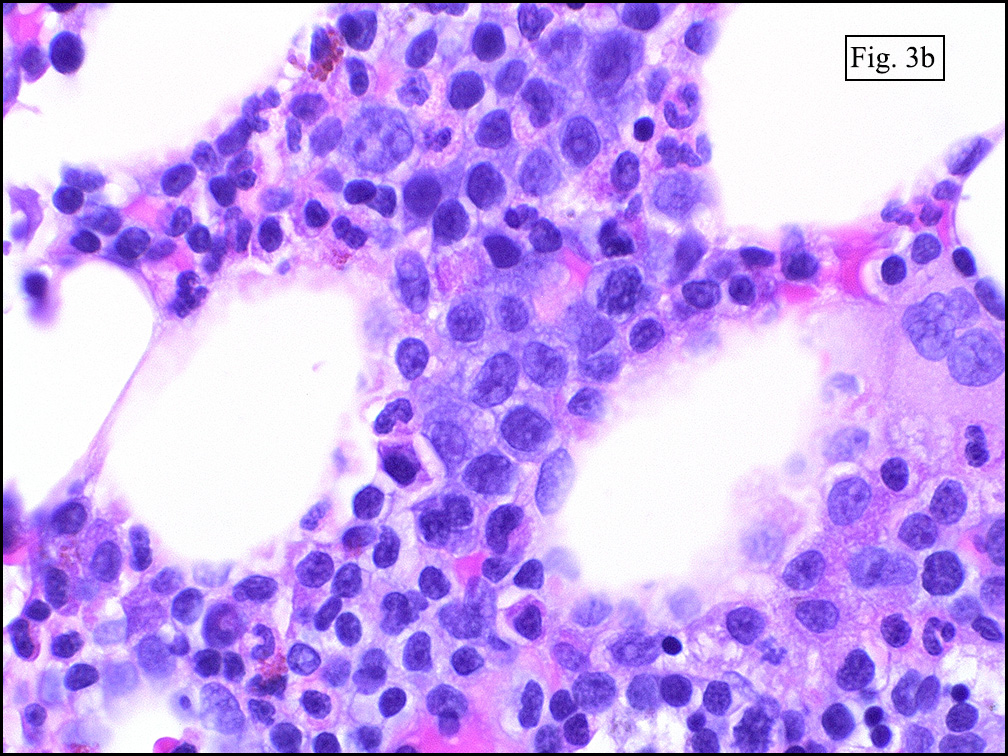
History: A 90-year-old man with a complex past medical history presented to the emergency department after a fall. He was found to have an elevated white cell count (36 x 109/L) without monocytopenia which prompted blood smear review. The blood smear demonstrated frequent medium-sized lymphocytes with round, occasionally clefted nuclei with mildly condensed chromatin, prominent nucleoli, and moderate amounts of pale, basophilic cytoplasm showing multiple hair-like projections (Figs. 1a, 1b, 1c). Flow cytometry was performed on the peripheral blood and showed a kappa-restricted population of lymphocytes expressing CD19, CD20 (Fig. 2), FMC7, CD103, CD11c. A CD25 were negative. A bone marrow biopsy was subsequently performed and showed an immunophenotypically identical population comprising about 35% of bone marrow constituents (Figs. 3a, 3b).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Hairy cell leukemia variant
Laura Denham1, MD; Jeff Cao1, MD; Donald R. Chase1,2, MD
1. Department of Pathology and Human Anatomy, Loma Linda University
Medical Center, Loma Linda, California
2. California Tumor Tissue Registry, Loma Linda, California
Discussion: Hairy cell leukemia variant (HCLv) is a B-cell lymphoproliferative neoplasm first described by Cawley et al. in 1980 and later termed the “prolymphocytic variant†of hairy cell leukemia. It is a rare disorder, comprising approximately 10% of hairy cell leukemias and 0.4% of all chronic lymphoproliferative disorders, corresponding to about 60-75 cases per year in the United States. As described below, the name is somewhat of a misnomer, as this entity is no longer thought to be related to classic hairy cell leukemia. HCLv is currently a provisional diagnosis in the WHO 2008 and is categorized under “splenic lymphoma/leukemia unclassifiableâ€.
Patients with HCLv tend to present in their 60’s and 70’s with symptoms of abdominal discomfort secondary to splenomegaly. In addition, they may also complain of weight loss and weakness. Hepatomegaly is present in a subset of patients. There is a slight male predominance, but less so than in classic hairy cell leukemia (cHCL).
Laboratory findings include leukocytosis without monocytopenia. This picture is different than cHCL which generally demonstrates monocytopenia without lymphocytosis. Anemia and thrombocytopenia may also be present in some cases. Cytopenias appear to be the result of hypersplenism rather than bone marrow replacement by a malignant infiltrate.
In contrast to the rare and sometimes difficult to find hairy cells of cHCL, circulating hairy cells or HCLv usually comprise greater than 50% of nucleated cells within the peripheral blood. These cells exhibit moderate to abundant amounts of pale blue cytoplasm with hairy projections. The central, round nucleus commonly contains somewhat condensed chromatin and a prominent nucleolus. Clefted or irregular nuclei are occasionally seen.
Immunophenotypically, HCLv marks as mature B-cells, with expression of CD19, CD22 and FMC7. They are negative for CD10. Unlike cHCL, the variant form does not express CD25 or Annexin A1, and they variably express CD11c (~87% positivity), and CD103 (~60% positivity). Tartrate resistant alkaline phosphatase (TRAP) is also weakly or variably expressed. In regards to clonality, they are more commonly lambda light chain restricted than kappa light chain restricted.
Bone marrow examination shows a hypercellular marrow with an interstitial infiltration of neoplastic lymphoid cells. Involvement of these cells is typically of only a mild degree, and may be quite subtle. Occasional clusters or nodules may be present. Sinusoidal involvement has been reported, but is usually focal. In contrast to the cHCL, reticulin deposition is only slightly to moderately increased, resulting in an easily attainable aspiration when compared to the notoriously difficult aspiration of reticulin-laden cHCL. Splenic involvement typically causes red pulp expansion by neoplastic lymphoid cells with resulting white pulp follicle atresia.
The differential diagnosis for HCLv includes classic hairy cell leukemia, splenic diffuse red pulp small B-cell lymphoma and B-cell prolymphocytic leukemia.
• Classic hairy cell leukemia: As previously stated, monocytopenia may be present, however, lymphocytosis is negligible. There is a strong male predominance, and patients often present with signs of infection. The peripheral blood may show only rare, hairy cells. CD25 and Annexin A1 are positive in cHCL, and reticulin fibrosis is usually moderate to marked.
• Splenic diffuse red pulp small B-cell lymphoma (also known as splenic lymphoma with villous lymphocytes): This entity is also a provisional diagnosis in WHO 2008 characterized by a mild lymphocytosis composed of small lymphocytes with round nuclei displaying condensed chromatin and occasional small nucleoli. The cytoplasm is scanty, with villous projections. Plasmacytoid cytology may be seen. Bone marrow infiltrates predominately involve sinusoids, with occasional interstitial/nodular involvement. Splenomegaly is typical and shows diffuse red pulp expansion with absence of follicular replacement. The cells mark with CD20, DBA.44 and are negative for CD25, CD103, CD11c, CD123 and Annexin A1.
• B-cell prolymphocytic leukemia: Similarly to HCLv, patients often present with splenomegaly and leukocytosis. However, the lymphocytes of PLL demonstrate greater than 55% prolymphocytes which are of medium cell size, round nucleus with condensed chromatin and prominent nucleoli. The cytoplasm is scant and typically lacks projections. An interstitial or nodular infiltrate is seen in the bone marrow. In contrast to HCLv, splenic involvement is characterized by white pulp nodule expansion. Cells are positive for typical B-cell markers CD19, CD22, and FMC7.
The most important reason to differentiate HCLv from classic hairy cell leukemia is that the variant form does not respond to interferon α and has historically shown poor response to purine analogs (pentosin and cladribine) and alkylating agents (chlorambucil and cyclophosphamide). Patients have had better response to splenectomy, which decreases the volume of disease and improves the cytopenias caused by hypersplenism.
Like its classic counterpart, HCLv is has a chronic course with many patients succumbing to diseases other than their leukemia. The median survival for HCLv is about 9 years, compared to cHCL which is around 12 years. Rate of progression is low (~6%), and has been associated with p53 deletion. When transformed, patients present with abdominal masses, weight loss and fever. Circulating blasts are present with a phenotype similar to that seen in the peripheral blood at initial presentation.
In summary, hairy cell leukemia variant shows some features overlapping with classic hairy cell leukemia, such as hairy lymphocytes in the peripheral blood, expression of CD103 and CD11c in some cases and splenic involvement. However, there are notable differences between the two. The variant form presents with lymphocytosis without monocytopenia, and does not express CD25 or Annexin A1. In addition, there is lack of significant reticulin fibrosis within the bone marrow. Most importantly from a clinical perspective is the poor response of hairy cell leukemia variant to medications typically used to treat the classic from of hairy cell leukemia.
Suggested Reading:
1. Charin Y, Brandwein J, Pantalony D, Chang H. Hairy cell leukemia variant with features of intrasinusoidal bone marrow involvement. Arch Pathol Lab Med. 2005; 129:395-398.
2. de Totero D, Tazzari PL, Raspardori D, di Celle PF, Carbone A, Gobbi M, Foa R. Phenotypic analysis of hairy cell leukemia: “variant†cases express the interleukin-2 receptor beta chain, but not the alpha chain (CD25). Blood. 1993;82(2):528-535.
3. Kanellis G, Garcia-Alonso L, Camacho FI, Garcia JF, Mollejo M, Montes-Moreno S, Garcia-Vela JA, Piris MA. Hairy cell leukemia variant. J Hematopathol. 2011;4:13-16.
4. Matutes E, Wotherspoon A, Brito-Babapulle V, Catovsky D. The nature history and clinic-pathological features of the variant form of hairy cell leukemia. Leukemia. 2001;15:184-193.
5. Matutes E, Wotherspoon A, Catovsky D. The variant form of hairy-cell leukemia. Best Practice and Research Clinical Haematology. 2003;16(1):41-56.
6. Piris M, Foucar K, Mollejo M, et al. (2008) in WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, Splenic B-cell lymphoma/leukaemia, unclassifiable, eds Swerdlow SH, Campo E, Harris NL,et al. (IARC Press, Lyon, France), pp 191–193.
7. Sainati L, Matutes E, Mulligan S, de Oliveira MP, Rani S, Lamper IA, Catovsk D. A variant form of hairy cell leukemia resistant to α-interferon: clinical and phenotypic characteristics of 17 patients. Blood. 1990;76(1):157-162.