History: A 37-year-old healthy man presented with fever and mild abdominal discomfort and was subsequently found to have an enlarged spleen. Upon removal, the spleen was noted to have a spongy cut surface with multiple, variably sized hemorrhagic nodules.
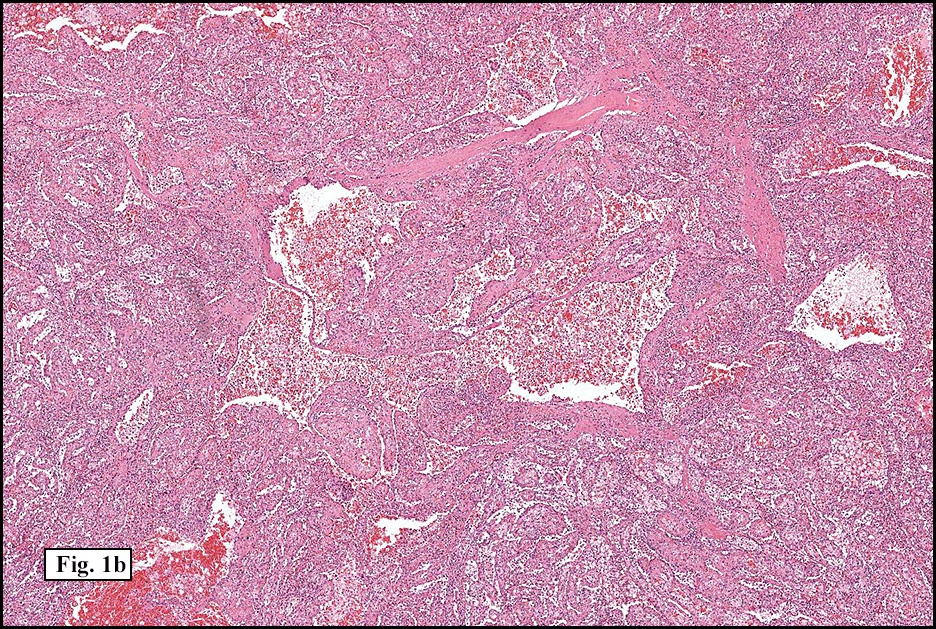
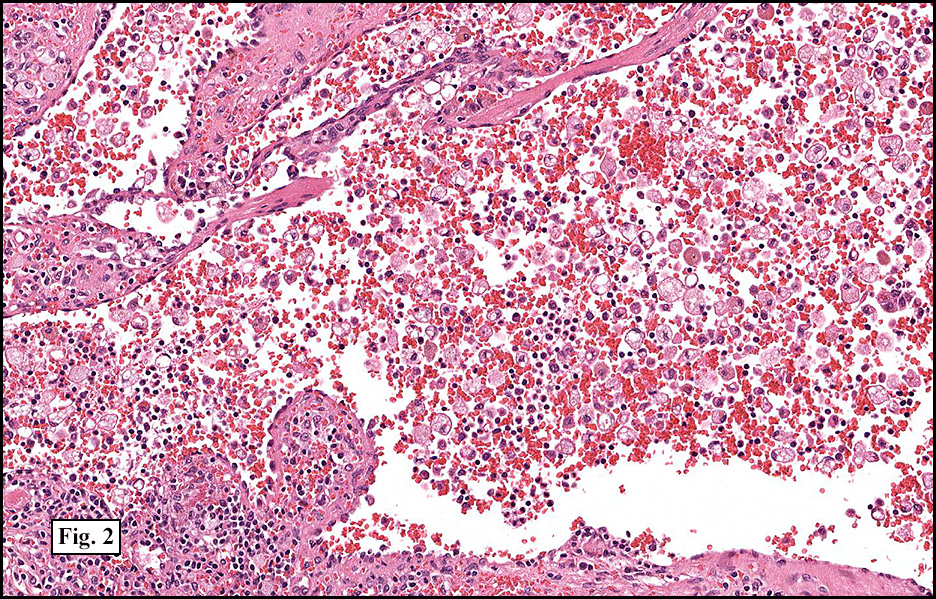
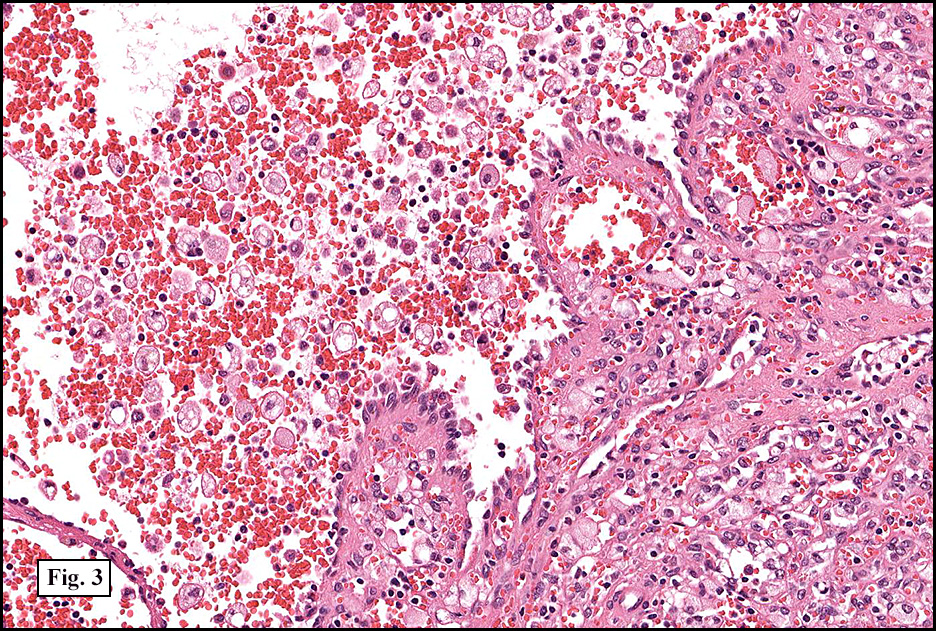
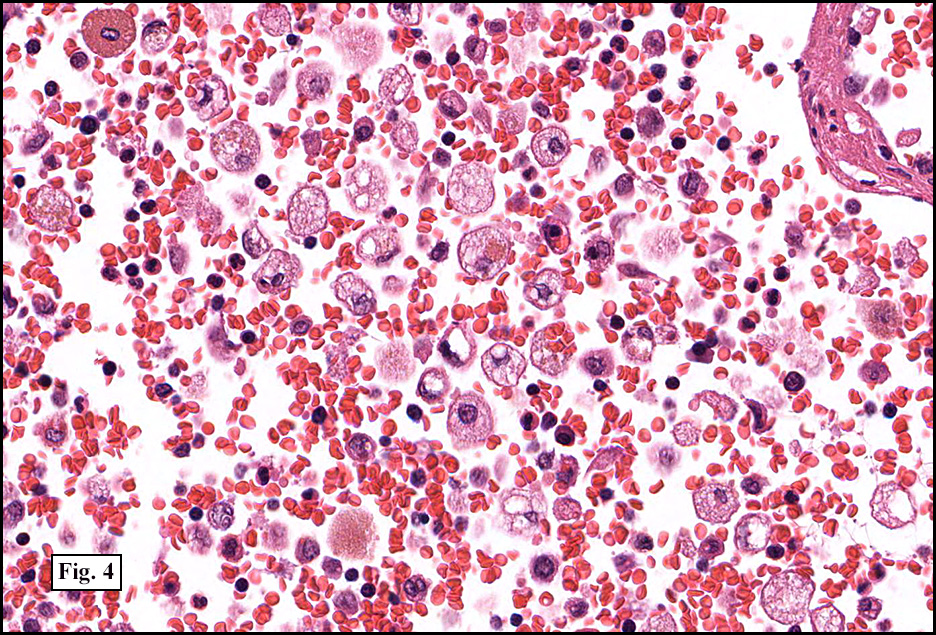
Microscopically, the nodules were comprised of anastomotic narrow and dilated vascular channels (Figs. 1a, 1b) with some areas forming pseudopapillary fronds (Figs. 2, 3). The vascular channels and pseudopapillary formations were lined with cytologically bland, tall endothelial cells, some of which had exfoliated into the vascular lumina (Fig. 3). The cells usually had vesicular to reniform nuclei, with occasional cells demonstrating hemophagocytosis and/or cytoplasmic eosinophilic globules (Fig. 4). Neither significant nuclear atypia nor significant mitotic activity was seen. Necrosis was not encountered. The tumor was positive for vascular marker CD31 and histiocytic marker CD68.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Littoral Cell Angioma, Spleen
Elif L. Akin, M.D. and Donald R. Chase, M.D.
Department of Pathology & Human Anatomy
Loma Linda University Medical Center, Loma Linda, California
Discussion: Originally described in 1991 by Falk et al, littoral cell angioma (LCA) is a benign vascular neoplasm that occurs exclusively in the spleen. It is thought to arise from the spleen’s littoral cells which line the sinuses of the red pulp. LCA has no penchant for either gender or age and has been described in infants as well as in adults. Although LCA is occasionally diagnosed incidentally, patients typically present with fevers, anemia, and/or thrombocytopenia along with splenomegaly. Symptoms, when present, typically resolve following splenectomy.
Grossly, LCA usually forms well-circumscribed spongy, hemorrhagic nodules in the splenic red pulp. These nodules may be solitary but are most often multiple and range in size from 0.1 to 9.0 cm. The nodules of LCA may compress and even replace adjacent normal splenic parenchyma.
Microscopically, LCA is characterized by variably sized anastomosing vascular spaces with occasional cystic spaces and pseudopapillary fronds projecting into lumina. The cells lining the vascular spaces are mostly tall with vesicular and sometimes reniform nuclei. Nucleoli, when seen, are inconspicuous. The tumor cells contain ample cytoplasm, some with eosinophilic globules, and may project and exfoliate into the vascular lumina. Hemophagocytosis is often present. No significant nuclear pleomorphism, mitotic activity, or necrosis is present.
LCA has a distinct immunophenotype, demonstrating dual reactivity for endothelial and histiocytic markers. Generally, it expresses Factor VIII, CD31, CD68, CD163, and CD21. Of note, LCA does not express CD34 or CD8. That LCA lacks expression of CD8 is rather curious, as this marker has been shown to be positive in normal littoral cells. Because of this, some authors have suggested that LCAs actually do not arise from littoral cells, however, no convincing alternative has been presented.
Interestingly, in spite of the belief that LCA is a benign neoplasm, some authors have noted a possible association with malignancy in up to a third of patients, suggesting that LCA may be a part of a clinical syndrome. At this time, further studies are required.
The differential diagnosis includes a variety of benign and malignant vascular neoplasms:
• Angiosarcoma is rare in the spleen and is characterized by poorly demarcated and infiltrative nodules. It shows a more haphazard growth pattern than LCA and has significant cytologic atypia, increased mitotic activity and necrosis.
• Hemangioendothelioma has features somewhere in-between hemangioma and angiosarcoma. Although this intermediate grade malignancy has an immunophenotype virtually identical to that of LCA, it may be distinguished by epithelioid cells which are not as vesicular as LCA. It may also show intracytoplasmic vacuoles containing red blood cells.
• Hemangioma is a benign tumor characterized by vessels lined by flat endothelial cells with inconspicuous nuclei.
• Although both lymphangioma and LCA may have vascular spaces that contain proteinaceous material, lymphangioma has flatter endothelium and occasionally a tufted growth pattern.
• Vascular hamartoma is comprised of cytologically bland cells surrounded by red pulp-like stroma with lymphocytic aggregates associated with vessels. Unlike LCA, splenic vascular hamartomas express CD8.
In summary, littoral cell angioma is a benign neoplasm that occurs exclusively in the spleen. Patients usually present with multinodular splenomegaly which may be associated with hypersplenism and is cured by splenectomy. This neoplasm is thought to arise from the sinus lining cells of the splenic red pulp and it is characterized by anastomosing vascular channels with tall endothelial cells, pseudopapillary projections, hemophagocytosis, and cells sloughed into the vascular lumina. The neoplastic cells express dual reactivity for endothelial and histiocytic markers (CD31, CD68) but do not express CD34 or CD8. LCA has been associated with visceral malignancies; therefore, close clinical follow-up is advised for patients with this diagnosis.
Suggested Reading:
Arber DA, Strickler JG, Chen Y-Y, Weiss LM. Splenic vascular tumors: a histologic, immunophenotypic, and virologic study. Am J Surg Pathol 1997; 21:827-835.
Bisceglia M, Sickel JZ, Giangaspero F, Gomes V, Amini M, Michal M. Littoral cell angioma of the spleen: an additional report of four cases with emphasis on the association with visceral organ cancers. Tumori 1998; 84: 595-9.
Dascalescu CM, Wendum D, Gorin NC. Littoral-Cell Angioma as a Cause of Splenomegaly. N Engl J Med 2001; 345(10): 772.
Falk S, Stutte HJ, Frizzera G. Littoral cell angioma: a novel splenic vascular lesion demonstrating histiocytic differentiation. Am J Surg Pathol 1991; 15(11): 1023-1033.
Fernandez S, Cook GW, Arber DA. Metastasizing splenic littoral cell hemangioendothelioma. Am J Surg Pathol 2006; 30(8): 1036-1040.
Fletcher CD. Diagnostic Histopathology of Tumors (3rd ed). Churchill Livingstone Elsevier. 2007: 1305-1307.
Veillon DM, Williams RB, Sardenga LJ, Harrison GK, Cotelingam JD. ‘Little’ Littoral cell angioma of the spleen. Am J Surg Pathol 2000; 24(2): 306-307.