History: Two years earlier, a now 54 y/o old man was diagnosed as having a schwanomma in his left arm. It was excised, but now he presented with a recurrent subcutaneous mass in the same location. The excised mass was 40 grams, 6.5 x 4.5 x 4.0 cm. The tumor was solid, firm and white-yellow.
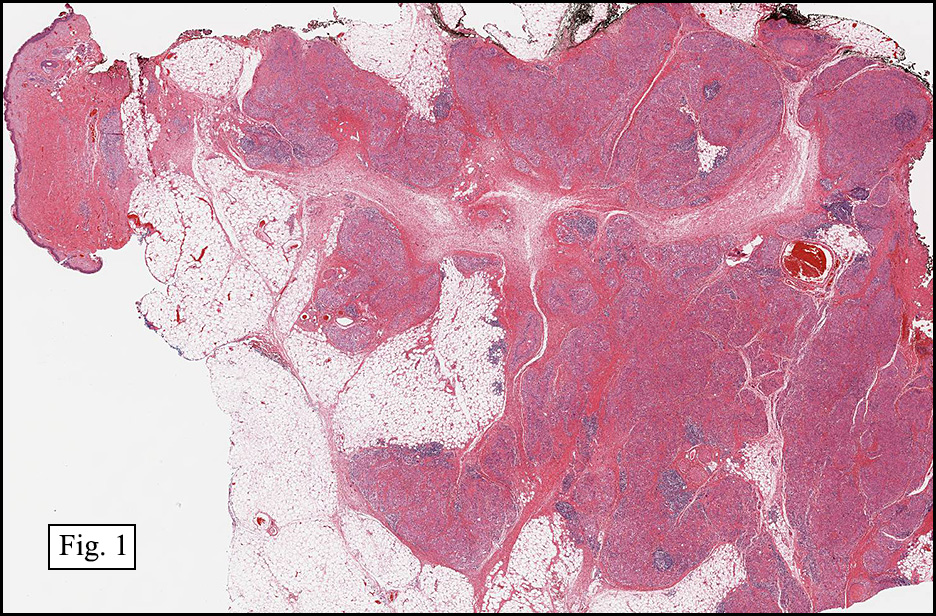
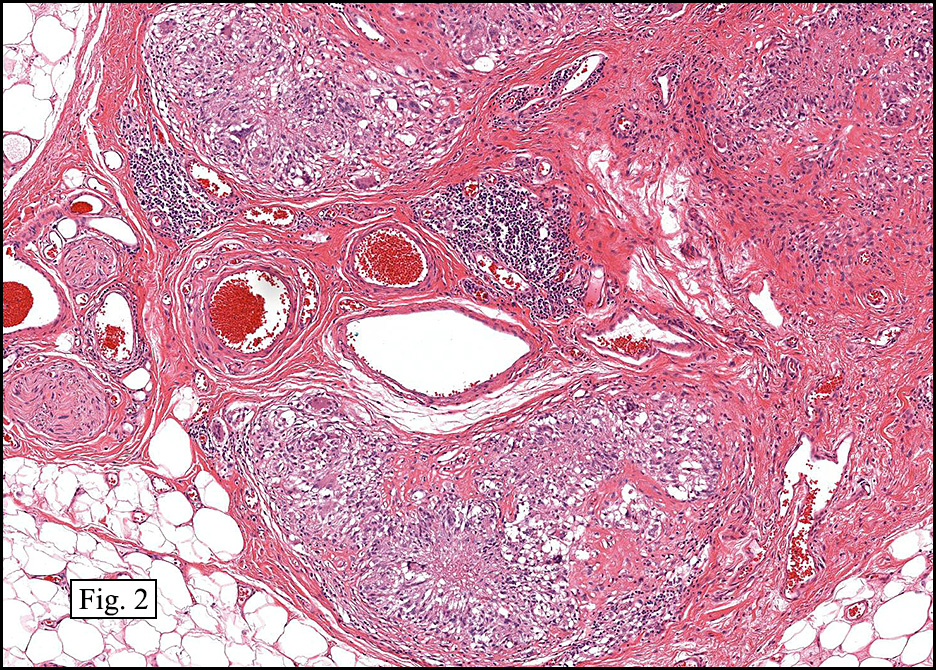
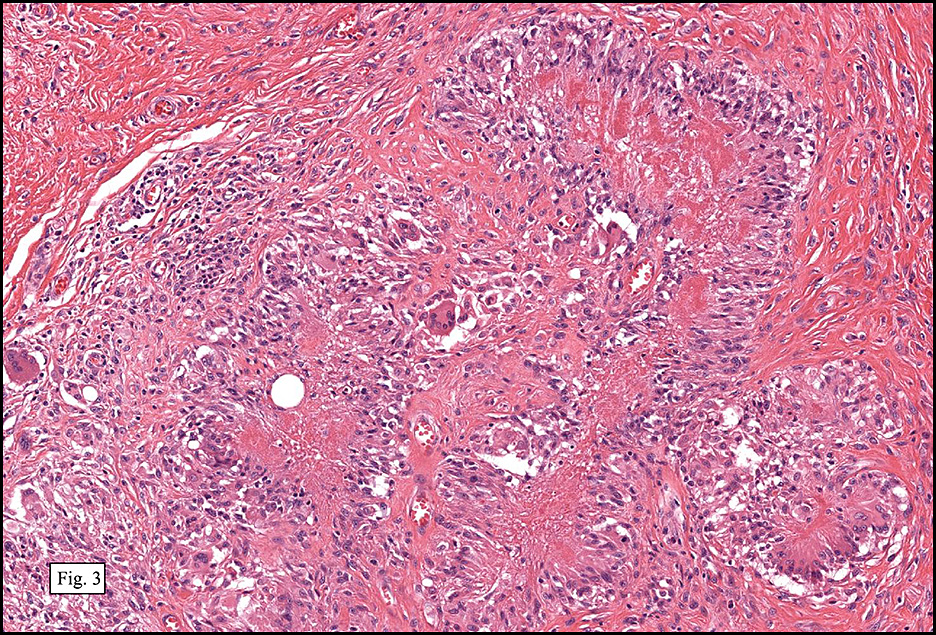
Microscopically, the mass was generally circumscribed but had fibrous extensions into the fat. The confluent fibrous bundles formed septae, giving a plexiform appearance (Fig. 1). Inside the septae were numerous multinucleated giant cells, plump mononuclear histiocyte-like cells with abundant eosinophilic cytoplasm, cigar-shaped nuclei and prominent small nucleoli (Fig. 2). The histiocyte-like cells lined up in a palisading pattern in some areas (Fig. 3). Lymphocytes and plasma cells were also seen either singly or in small clusters. Dilated blood vessels were common (Fig. 2). No mitoses, necrosis nor significant pleomorphism were seen. The overlying skin was normal.
{kind=link}
{kind=link}
{kind=link}
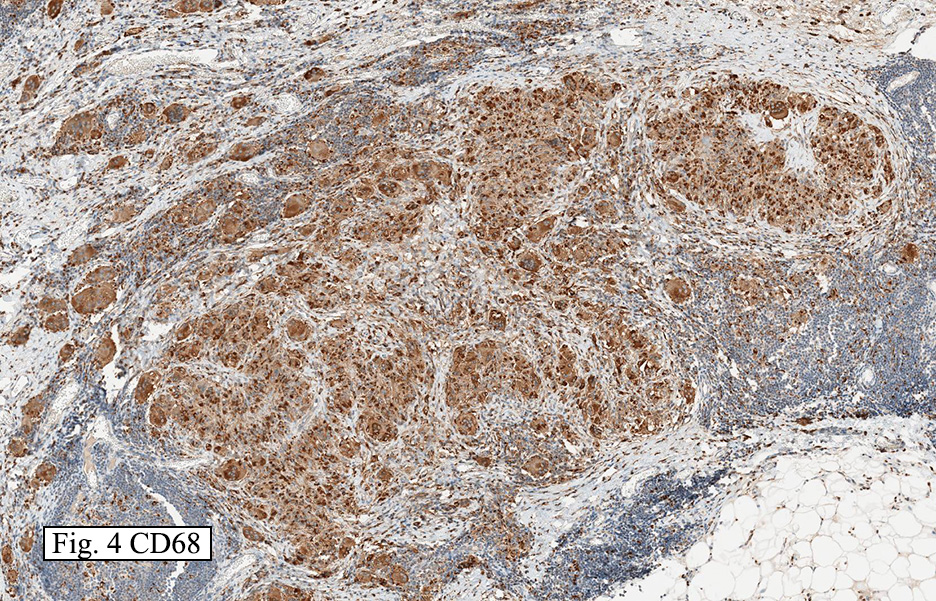
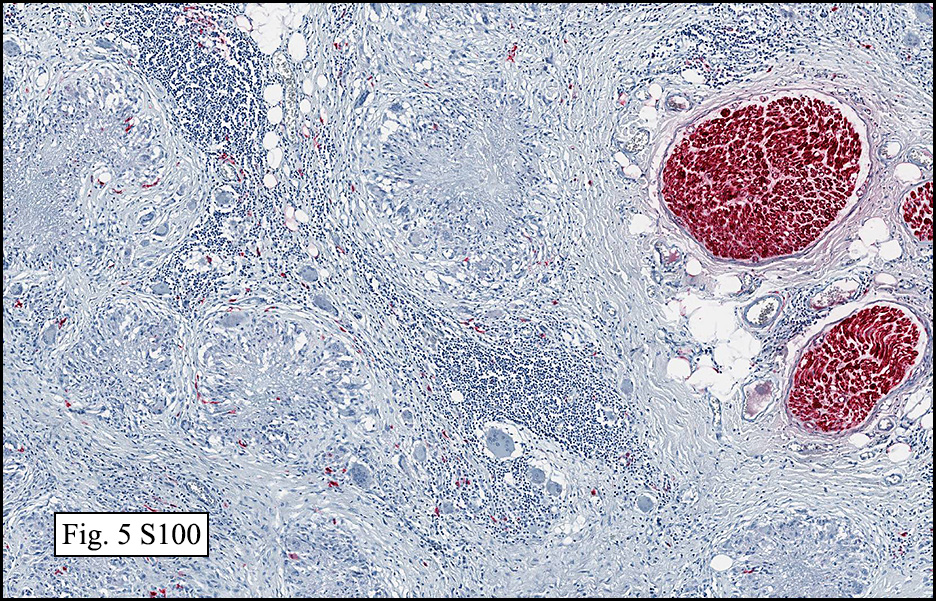
Immunohistochemical stains showed the giant cells and histiocyte-like cells to be strongly positive for CD68 (Fig. 4), but negative for S-100 (Fig. 5) and cytokeratin.
{kind=link}
{kind=link}
Diagnosis: Plexiform Fibrohistiocytic Tumor (Plexiform Fibrous Histiocytoma)
Bingbing Song, M.D. and Donald R. Chase, M. D.
Department of Pathology & Human Anatomy
Loma Linda University Medical Center,
Loma Linda, California
Discussion: Plexiform fibrohistiocytic tumor (PFT) is composed of network of fibrocytes alternating with nodules of giant cells, histiocytes, and chronic inflammatory cells. Though the tumor mostly usually occurs in female patients younger than 30 years, one third have been reported in children less than 10 years old. A small number have also been reported in older patients. The WHO views these tumors as being of “intermediate gradeâ€.
PFTs are usually slowly growing, solitary, painless nodules that have a propensity to occur in the upper arm. They are usually located in the subcutis and are 1-3 cm in diameter. Their cut surface is usually gray-white and firm.
A striking microscopic feature is bundles of fibrous tissue forming a syncytium, with scattered regions of giant cells and mononuclear histiocyte-like cells. These elements are present in varying amounts resulting in three subtypes:
• Fibrohistiocytic subtype: composed mainly of nodules of mononuclear histiocyte-like cells and multinucleated giant cells.
• Fibroblastic subtype: composed mainly of elongated clusters and short fascicles of fibroblast-like cells
• Mixed subtype: composed of both patterns in equal proportion.
The tumor generally forms long extensions which radiate into the surrounding soft tissue. The fibrous tissue is composed of spindled fibrocytes with small nuclei. Nodules are composed of either exclusive histiocyte-like cells or a mixture of histiocyte-like cells and osteoclast-like multinucleated giant cells. The histiocyte-like cells can be either plump/round or spindled with plenty eosinophilic or pale granular cytoplasm. Hemorrhage and hemosiderin are common in the nodules and help to identify this lesion. Chronic inflammation of plasma cells and lymphocytes is often present around the nodules. Dilated blood vessels can be prominent in the tumor, especially in the fibrous tissue. Cellular atypia and pleomorphism are minimal. Mitotic activity is often every low. Vascular invasion is observed in 10-20% of cases. The giant cells and histiocytes-like cells are positive for CD68, and negative for S-100, keratin, factor VIII and CD45. Fibroblasts decorate for vimentin and smooth muscle actin.
PFTs often recur locally, but rarely metastasize. When metastatic to the lung, small fibrohistiocytic nodules usually are found in subpleural locations and/or peribronchiolar regions.
The differential diagnosis includes a variety of fibroblastic/fibromyoblastic tumors and nerve tumors of the soft tissue.
• Plexiform Schwannoma (PS) also has a plexiform pattern and nuclear palisading. But the cells in the nodules are more spindled with no giant cells present. Unlike PFH, PS is strongly positive for S-100.
• Neurothekeoma (NT) also displays a plexiform pattern and is located subcutaneously. But the nodules mostly contain spindle cells instead of plump histiocyte-like cells. Usually the cellularity in the nodules is lower and the stroma is more myxoid with no giant cells seen. These cells express S-100, but not CD68. Some neurothekeomas are more cellular and strongly positive for CD68 but not S-100. This variant of NT has been suggested to have a common histogenesis as PFH.
• Benign dermal and subcutaneous fibrous histiocytomas may contain foam cells and are better circumscribed than PFH.
• Fibrous hamartoma of infancy generally occurs in the similar age group. However, the tumor contains primitive cells within a unique myxoid stroma (“organoid bodiesâ€), but does not have giant cells.
• The absent pleomorphism and rare mitotic activity help to differentiate PFT from
Atypical fibroxanthoma,
Giant cell sarcoma of soft parts, and
Pleomorphic MFH (Pleomorphic Sarcoma).
In summary, plexiform fibrous histiocytoma is an intermediate grade, subcutaneous tissue tumor with a fibrous network containing nodules of giant cells, histiocyte-like cells and intermixed chronic inflammation. The tumor cells strongly express CD68, but not S-100, cytokeratin or factor VIII. It often recurs but rarely metastasizes.
Suggested Reading:
Fletcher CDM, Unni KK, Mertens F, et al. World Health Organization Classification of Tumors, Pathology and Genetics Tumors of Soft Tissue and Bone. 2002.
Kempson RL, Fletcher CDM, Evan HL, et al. Atlas of Tumor Pathology, Tumors of the Soft Tissue. 3rd series, 1998.
Moosavi C, Jha P, Fanburg-Smith JC. An update on plexiform fibrohistiocytic tumor and addition of 66 new cases from the Armed Forces Institute of Pathology, in honor of Franz M. Enzinger, MD. Ann Diagn Pathol. 2007; 11(5): 313-9.
Taher A, Pushpanathan C. Plexiform fibrohistiocytic tumor: a brief review. Arch Pathol Lab Med. 2007; 131(7): 1135-8.
Jaffer S, Ambrosini-Spaltro A, Rosai J, et al. Neurothekeoma and plexiform fibrohistiocytic tumor: mere histologic resemblance or histogenetic relationship? Am J Surg Pathol. 2009;33(6):905-13.