History: A 58 year-old woman with a 6 year history of dermatomyositis presented with a 7 month history of a painless 1.5 x 1.0 cm skin ulcer near her right elbow on the dorsal surface of the proximal forearm. She had a 6 year history of methotrexate (MTX) treatment during which time other cutaneous wounds had arisen, but unlike this one, had healed. Physical examination also showed decreased muscle strength in her shoulder and hip flexors, but neither lymphadenopathy nor hepatosplenomegaly were identified.
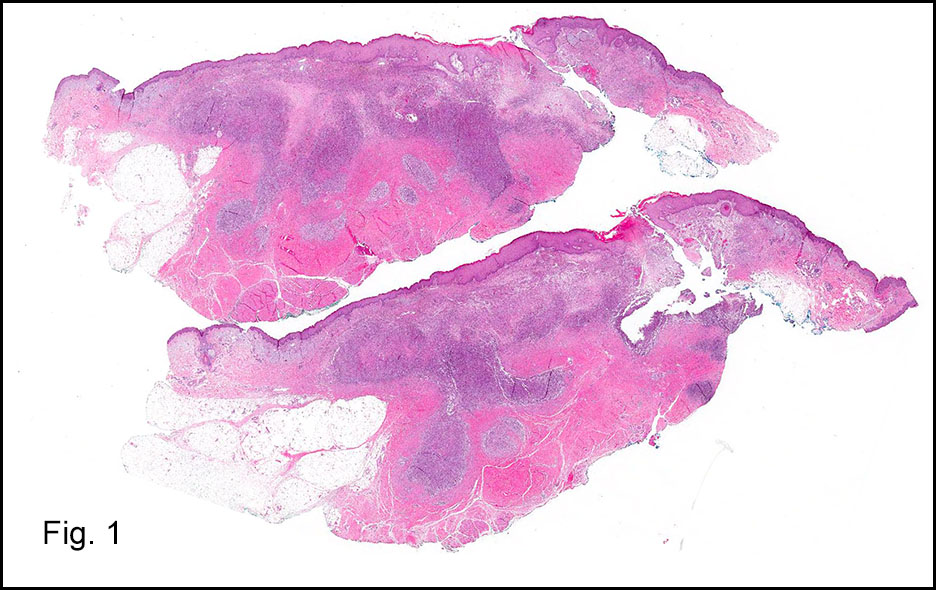
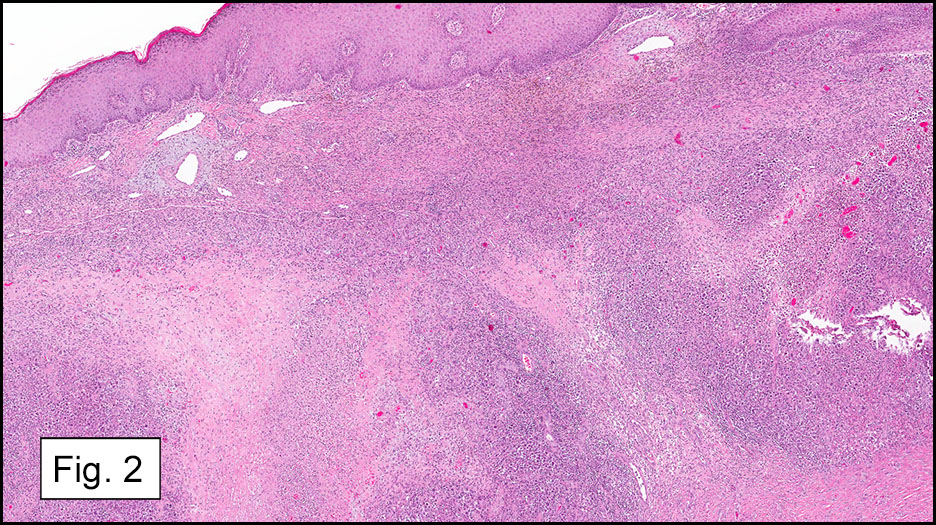
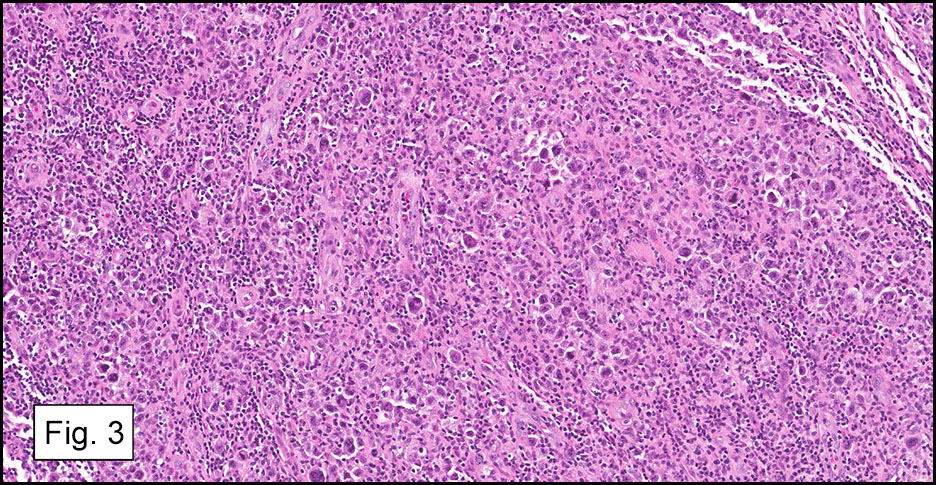
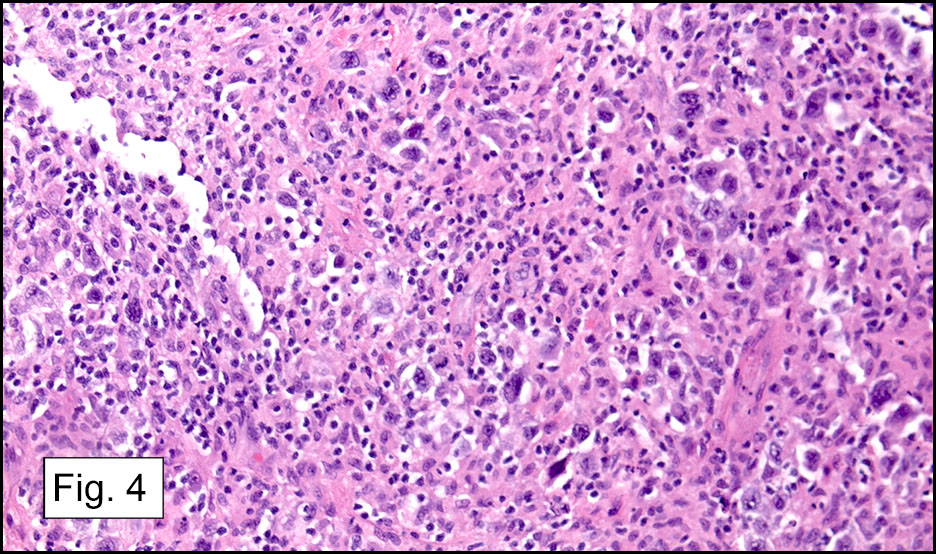
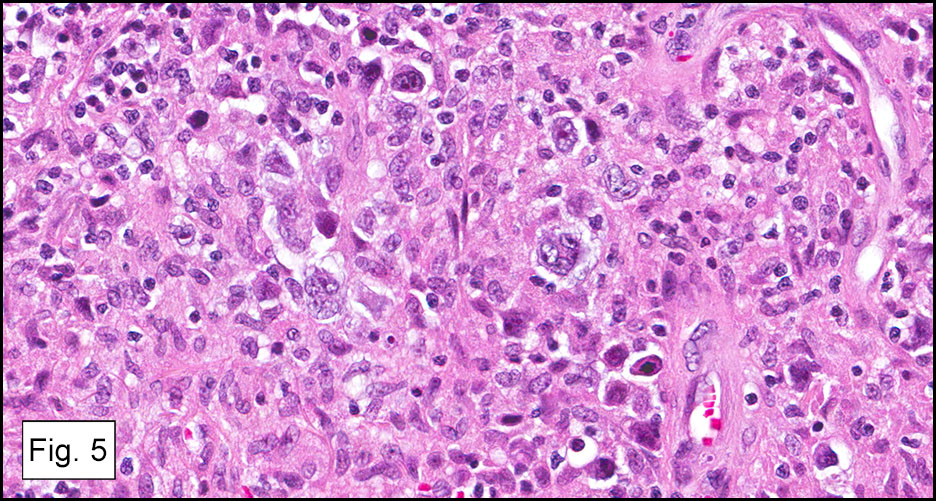
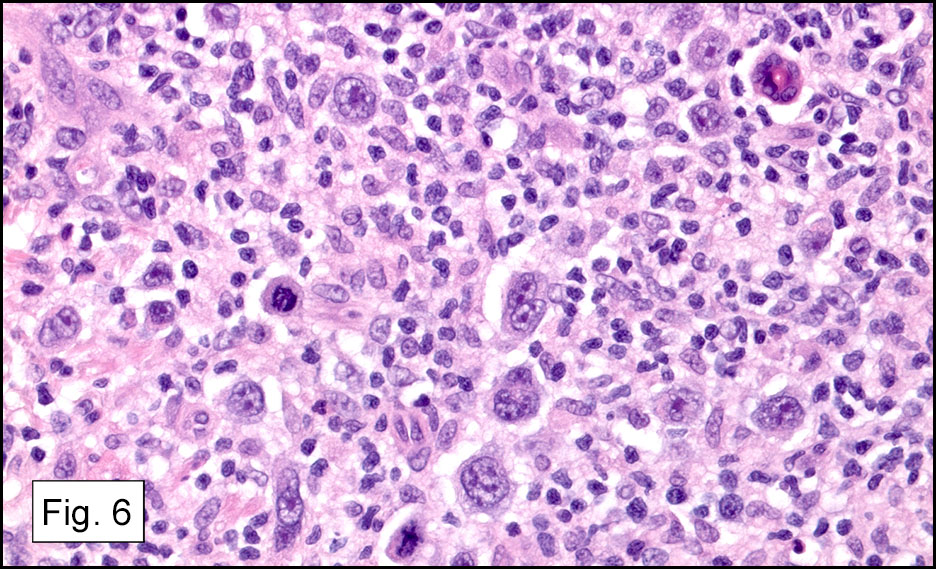
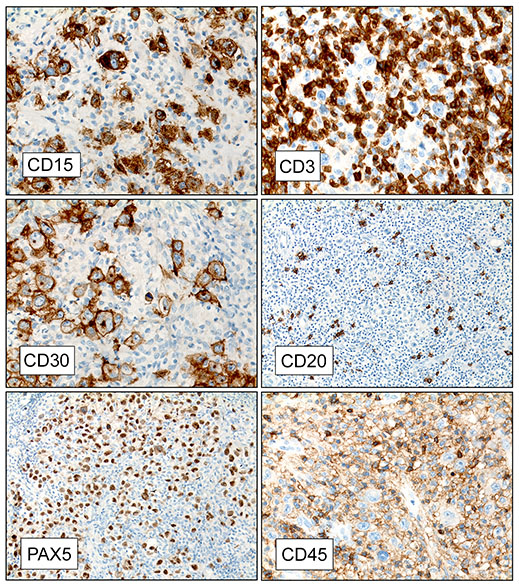
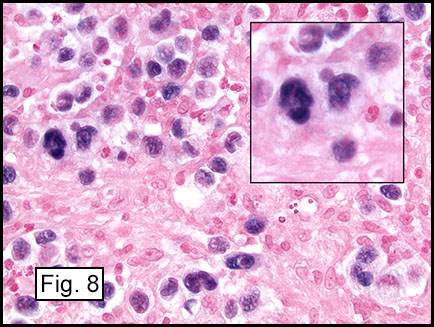
Microscopically the mass was centered in the dermis (Figs. 1,2) and consisted of hypercellular, sheet-like dermal infiltrates (Figs. 3,4). The infiltrate was particularly noteworthy for scattered atypical cells with large bi- or mono-lobed nuclei. These cells also had pale vesicular chromatin, amphophilic cytoplasm and were felt to be Reed-Sternberg (RS) cells and variants (Figs. 5,6). Admixed with them were small lymphocytes, plasma cells, neutrophils and rare eosinophils. The RS cells and variants stained positive for CD15, CD30, and PAX-5, but negative for CD3, CD20 and CD45 (Fig. 7). An Epstein-Barr virus (EBV) staining by EBER in-situ hybridization was positive in the RS cells/variants (Figs. 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
After withdrawing MTX therapy the site healed well, and the patient was spared additional chemotherapy and radiation. However after 13 months the tumor recurred locally at the same location.
Diagnosis: Primary Cutaneous Hodgkin Lymphoma Presenting as an Epstein-Barr Virus Positive Methotrexate-associated Lymphoproliferative Disorder
Ying Zhao, MD; Ravi Raghavan, MD; Jun Wang, MD; Donald R Chase, MD
Department of Pathology and Human Anatomy,
Loma Linda University Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion:
There are only a few reported cases of Hodgkin lymphoma (HL) presenting as a primary cutaneous lesion (Mukesh et al). Patients are usually in the terminal phase of the disease and have already sustained extensive systemic and lymph node involvement.
According to the 2008 WHO classification of tumors of hematopoietic and lymphoid origin, our case presentation tumor falls into an iatrogenic subgroup of immunodeficiency-associated lymphoproliferative disorders (LPD). In fact, MTX was the first reported agent associated with LPD, noticed when it occurred in patients being treated for rheumatoid arthritis (RA). The frequency of this relationship is not well known. In one large survey, 478 lymphoma cases were recorded among 101,589 patients treated with methotrexate and/or anti-TNF therapy for RA (Wolfe et al.). Among the MTX-LPD, 40-50% were extranodal, including gastrointestinal tract, skin, liver, spleen, lung, kidney, thyroid gland, bone marrow and soft tissue (Hoshida et al). According to the WHO classification, MTX-LPD mainly consists of diffuse large B-cell lymphoma (35-60%) and classical Hodgkin lymphoma (12-25%). Overall, 40% MTX-LPD were EBV positive, with EBV detected more frequently in Hodgkin lymphoma (~80%) than in DLBCL (~25%) or other B-cell lymphoma types. The hypothesis of pathogenesis of MTX-LPD is that the immunosuppressive state induced by MTX administration might contribute to development of LPD. It’s also noteworthy that patients with RA may have a T-lymphocyte defect that allows EBV-infected B-lymphocytes to survive.
In this case report, the tumor cell morphology and immunophenotype demonstrate classical Hodgkin lymphoma, which is associated with MTX treatment for the dermatomyositis and has EBV positivity. The differential diagnosis mainly includes cutaneous CD30+ lymphoproliferative disorders as listed below:
• Hodgkin lymphoma-like post-transplantation lymphoproliferative disorder (PTLD), is mainly seen in immunosuppressed recipients following solid organ or bone marrow transplantation. HL-like PTLD cases are almost always positive for EBV, with the EBER present not only in the large atypical cells but also in a substantial subset of the associated bystander small lymphocytes (Wang et al). HL-like PTLD may be either nodal or extranodal. The large atypical RS-like cells express CD45 and B-cell markers (CD20 and/or CD79a) with variable expression of CD30 but not CD15. This entity shows an aggressive clinical course.
• Primary cutaneous anaplastic large cell lymphoma, is a CD30+ T-cell lymphoma presenting with skin nodules or ulceration with diffuse, non-epidermotropic infiltrates. The large CD30+ anaplastic tumor cells have the characteristic morphology of anaplastic cells, showing round, oval or irregularly-shaped nuclei, prominent eosinophilic nucleoli and abundant cytoplasm. The neoplastic cells express T-cell markers such as CD3, CD4, granzymeB and TIA, but are negative for CD15 and EBV.
• Mycosis fungoides with large cell transformation, is a tumor stage of MF and defined by presence of over 25% large lymphoid cells in the dermal infiltrates. With progression, the dermal infiltrates become more diffuse and epidermotropism may be lost. The large CD30+ transformed cells present as large cribriform cells or blast cells with prominent nucleoli. They generally express a T-cell phenotype as CD2+, CD3+, CD4+, but CD15 -.
• Lymphomatoid papulosis is a chronic, recurrent, self-healing papular or nodular skin lesion. The atypical cells can present as anaplastic, immunoblastic or Hodgkin-like cells, which are CD30+, CD15-, CD4+, and CD20- . Although this CD30 positive T-cell lymphoproliferative disorder has a malignant morphology, it is self-healing.
Spontaneous complete remission after cessation of MTX has been reported in DLBCL (up to 40%) and classical Hodgkin lymphoma (up to 30%) (Hoshida et al., Rita Rizzi et al.). The majority of responses occurred in EBV-positive cases and remission generally occurred within 4 weeks. In our case, despite positive margins, the patient went into remission for 13 months. Its recurrence, however, suggests the advisability to continue to monitor the patient for many months. Little is known about the interval for the recurrent tumor after initial spontaneous remission. It will be important to accumulate and evaluate many more cases of MTX-LPD and examine their clinical correlates.
Suggested Reading:
Mukesh M et al, Primary cutaneous Hodgkin’s lymphoma. Clin Exp Dermatol. 2009 Dec;34(8):e673-5.
Hoshida et al, Lymphoproliferative disorders in rheumatoid arthritis: Clinicopathological analysis of 76 cases in relation to methotrexate medication. .J Rheumatol. 2007 Feb;34(2):322-31.
Rita Rizzi et al, Spontaneous remission of ‘‘methotrexate-associated lymphoproliferative disorders’’ after discontinuation of immunosuppressive treatment for autoimmune disease.Review of the literature. Med Oncol (2009) 26:1–9.
Jun Wang et al. Hodgkin lymphoma-like post-transplantation lymphoproliferative disorder. Arch Pathol Lab Med. Vol130: 559-560
Wolfe F et al. The effect of methotrexate and anti-tumor necrosis factor therapy on the risk of lymphoma in rheumatoid arthritis in 19,562 patients during 89,710 person-years of observation. Arthritis Rheum 56:1433-1439.
Takemori N et al. Complete Remission of Methotrexate-Related Epstein-Barr-Virus-Associated Hodgkin-Like Lymphoma following Withdrawal of MTX Coupled with Clarithromycin Administration. Case Rep Hematol. 2012: 658745.
Satoh K et al. Reversible methotrexate-associated lymphoproliferative disorder resembling advanced gastric cancer in a patient with rheumatoid arthritis. Am K Med Sci. 2009 Oct: 338(4): 334-5.