 History: A 43-year-old male presented with a mass in his left mid-back that had been present for approximately two years. When excised, the mass was well-circumscribed and measured 5.5 x 4.0 x 2.5 cm. It was found to be superficial and did not involve bone or muscle.
History: A 43-year-old male presented with a mass in his left mid-back that had been present for approximately two years. When excised, the mass was well-circumscribed and measured 5.5 x 4.0 x 2.5 cm. It was found to be superficial and did not involve bone or muscle.
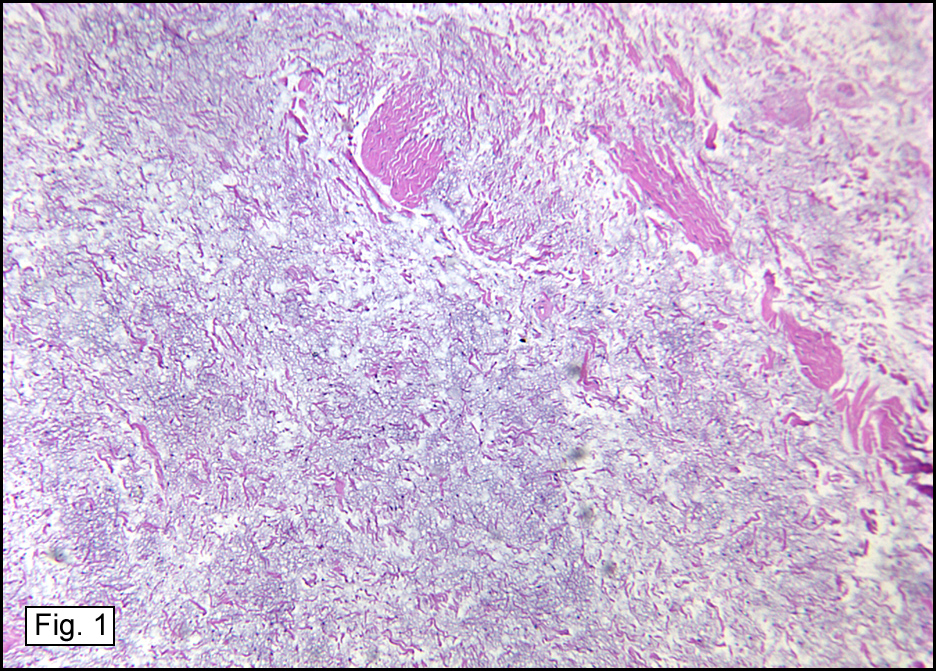
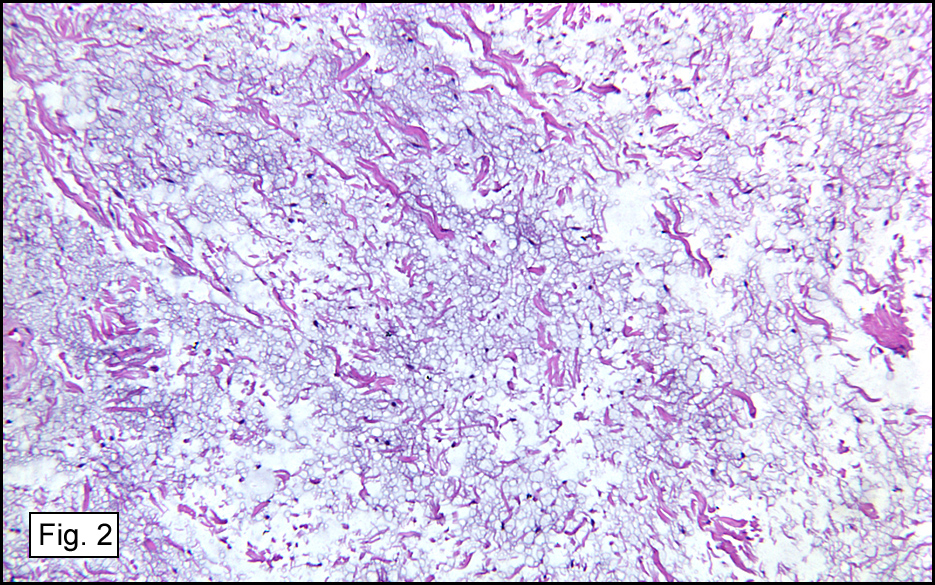
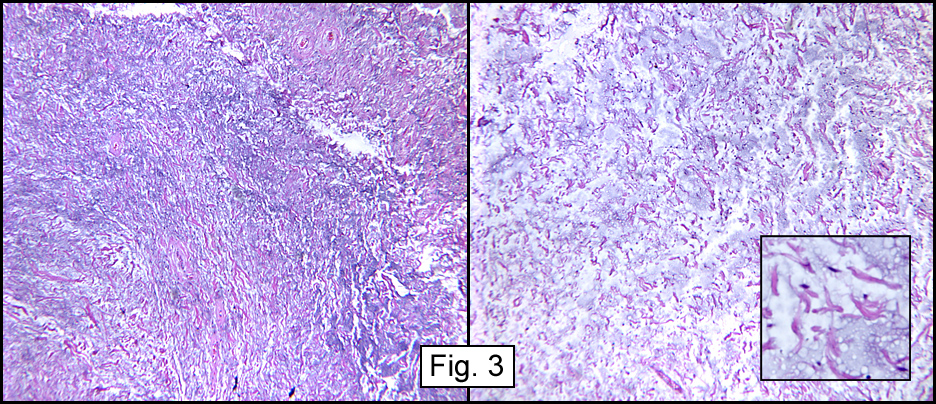
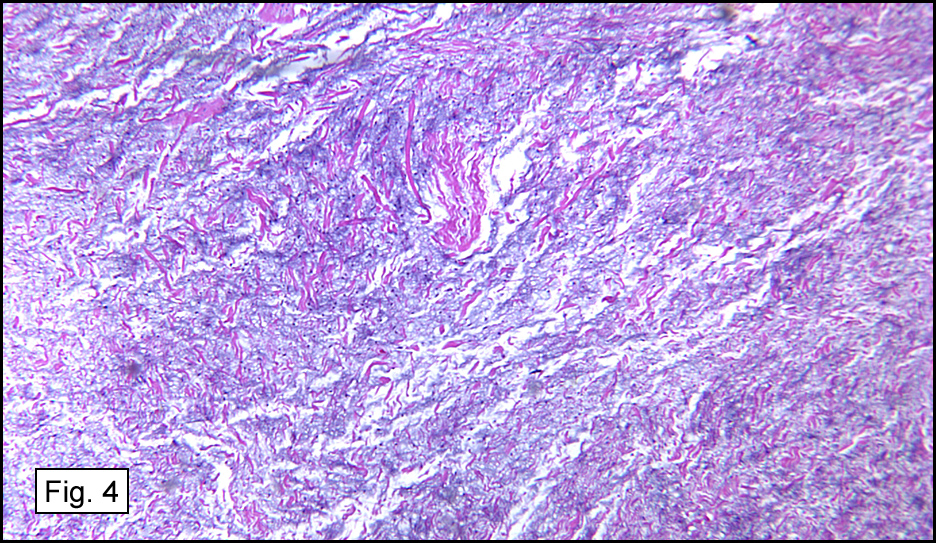
Microscopic examination showed a myxoid stroma containing bland spindled cells and hyalinized collagen (Fig. 1). The nuclei were uniform and small, and showed no cytologic atypia (Figs. 2,3,4). Blood vessels were infrequently encountered, and “staghorn†capillaries were not identified. Fatty elements were absent.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
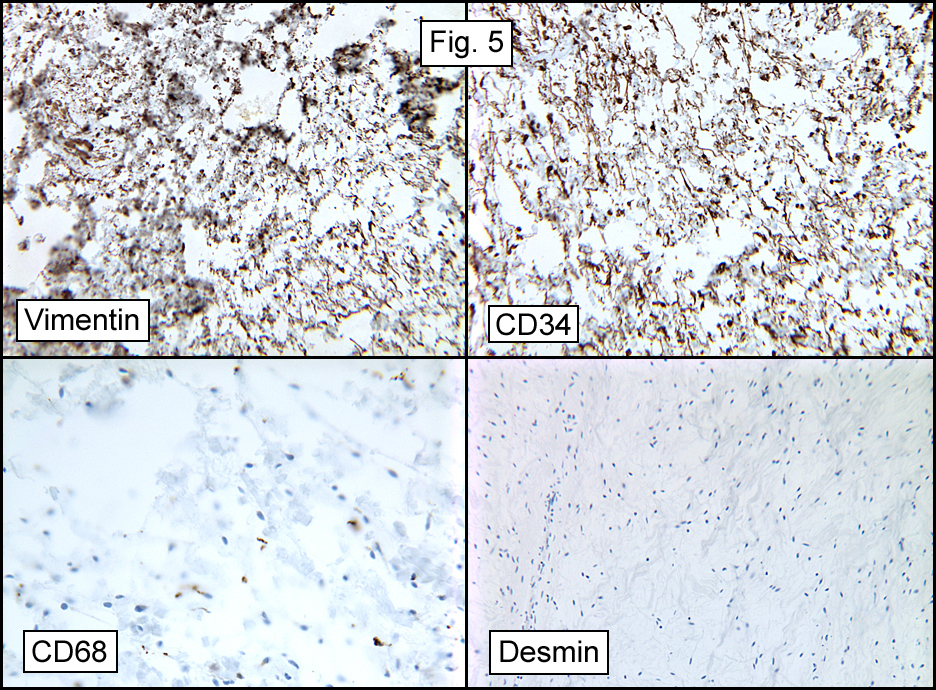
Immunostains showed strong decoration for vimentin and CD34 (Fig. 5). Stains for CD68, desmin, S100, muscle specific actin and smooth muscle actin were negative.
{kind=link}
Diagnosis: “Myxoid Spindle Cell Lipomaâ€
Brian Hutchins PSF, Donald R. Chase, M.D.
Department of Pathology, Loma Linda University and Medical Center
California Tumor Tissue Registry
Discussion: Originally described by Enzinger and Harvey in 1975, spindle cell lipoma (SCL) is a histologically distinct lesion characterized by an admixture of mature fat, collagen-forming spindle cells, and varying degrees of myxoid change.
The lesion has shown a male predilection with a presentation age of 45-60 years (mean 56). Although the tumor is unusual in adolescents and children, one report of SCL involved a 14-month-old girl. The tumors usually arise in the subcutaneous tissue of the posterior neck, shoulder, or back, but have also been described in the oral cavity, larynx, bronchus, breast, orbit and extremities. It manifests as a slow growing solitary, circumscribed or encapsulated painless firm nodule in the subcutaneous tissue. Multiple lesions are rare.
Grossly, the nodule usually resembles a fatty proliferation which varies somewhat in having either fibrous or gray-white gelatinous foci. Although some tumors are large (up to 14 cm), most are 3-5 cm. Microscopically, SCLs vary in appearance depending on the relative amounts of mature fat and spindle cells. Classically there is a relatively equal mixture of mature fat and spindle cells, however a spectrum exists. The spindled cells are uniform, with a single elongated nucleus and narrow, bipolar cytoplasmic processes. The nucleoli are inconspicuous as are mitotic figures. The cells may be haphazardly distributed but tend to be arranged in short parallel bundles often with striking nuclear palisading reminiscent of a neural tumor. In some cases scattered multinucleated floret-like giant cells, typical of those found in pleomorphic lipomas, are present. The cells are deposited in a mucoid matrix composed of hyaluronic acid and mixed with a varying number of birefringent collagen fibers. In some cases the tumors are highly myxoid and hypocellular with haphazardly arranged cells. Such cases may be confused with myxoma. The vascular pattern is usually inconspicuous and consists of a few small or intermediate-size thick-walled vessels.
Immunohistochemically, the spindle cells stain strongly for vimentin and CD34. S-100 protein does not mark the spindle cells, but mature lipocytes may show peripheral immunoreactivity. Actins (MSA and SMA), desmin, laminin, CD68 and monocyte/macrophage antigen MAC-387 are negative.
The differential diagnosis of SCL includes a variety of benign and malignant entities characterized by spindle cells deposited in myxoid stroma.
* Dermatofibrosarcoma protuberans (DFSP) is composed of a relatively uniform population of CD34+ spindle cells arranged in tight storiform patterns. However, DFSP tends to occur in younger patients, has a predilection to arise in the trunk and extremities, and histologically infiltrates the subcutaneous tissue in a characteristic honeycomb pattern.
* Given the striking nuclear palisading present in some spindle cell lipomas and the conspicuous mast cell infiltrate, schwannoma and neurofibroma are diagnostic considerations. The cells of these benign peripheral nerve sheath tumors tend to be more wavy or buckled in appearance; although both lesions may express CD34, and neural tumors commonly express S-100 protein, a marker that is negative in spindle cell lipoma. Some neural tumors also show Wagner-Meissner body formation, a feature lacking in SCLs.
* Myxoid liposarcoma is also in the differential as some spindle cell lipomas have a prominent plexiform vascular pattern in the myxoid areas. However, SCL is more circumscribed and is more superficially located than myxoid liposarcoma, It lacks lipoblasts and has ropey collagen bundles.
* Myxoid malignant fibrous histiocytoma (myxofibrosarcoma) is characterized by a prominent and bizarre nuclear atypia and has a coarse vasculature.
* Cutaneous myxoma is composed of a sparsely cellular proliferation of stellate and spindle-shaped cells deposited in an abundant myxoid matrix.
* Myxoid leiomyoma composed of widely scattered smooth muscle cells in a myxoid matrix arranged in small packets or loose fascicles.
Suggested Reading:
Enzinger and Weiss’s Soft Tissue Tumors (4th ed., Editors Weiss SW & Goldblum J), Mosby, pp 590-597, 2001.
Fletcher C, Unni K, Mertens F. In: Pathology and Genetics of Tumours of Soft Tissue and Bone, IARC Press Lyon, pp 31-35, 2002.
Miettinen M. Diagnostic Soft Tissue Pathology, Churchill Livingstone, pp 215-216, 2003.
Kempson R, et al, Tumors of the Soft Tissues (Third Series), AFIP, pp 203-208, 2001.
Angervall L, Dahl I, Kindblom LG, et al. Spindle cell lipoma. Acta Pathol Microbiol 84:477, 1976.
Enzinger, FM, Harvey, DA. Spindle cell lipoma. Cancer 36:1852, 1975.
Kitano M, Enjoji M, Iwasaki H. Spindle cell lipoma – a clinicopathologic analysis of 12 cases. Acta Pathol Jpn 29:891, 1979.