 History: A previously healthy 80 year-old man presented with a one-month history of right axillary lymphadenopathy. Physical examination revealed a mildly tender, firm, two cm lymph node in the right axilla. No other lesions identified.
History: A previously healthy 80 year-old man presented with a one-month history of right axillary lymphadenopathy. Physical examination revealed a mildly tender, firm, two cm lymph node in the right axilla. No other lesions identified.
Imaging studies confirmed the presence of an enlarged lymph node in the right axilla. There were no other radiological abnormalities.
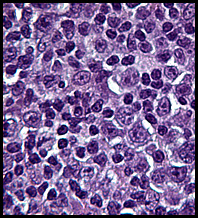
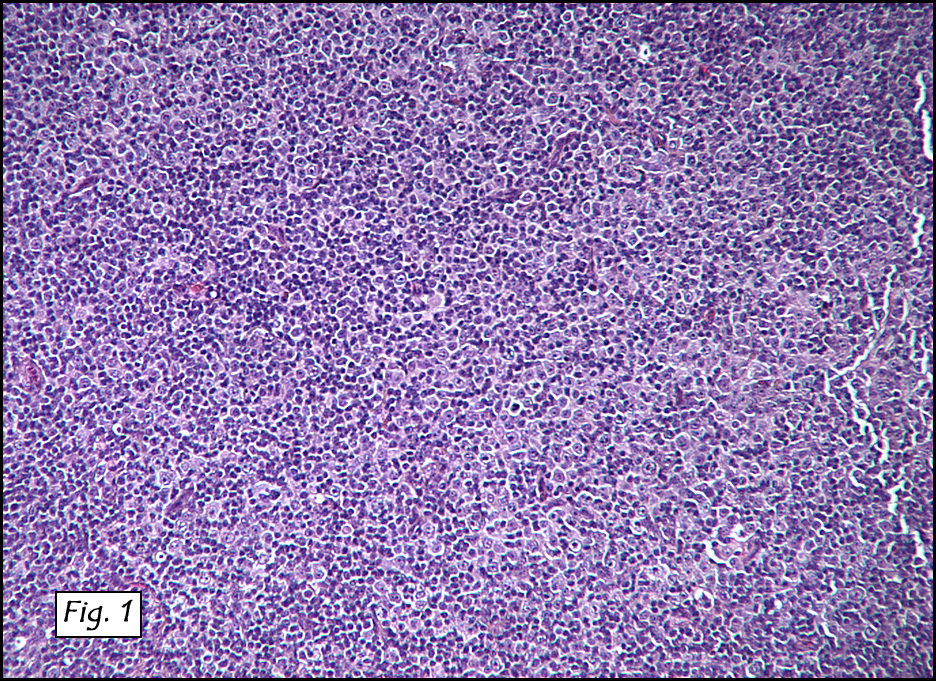
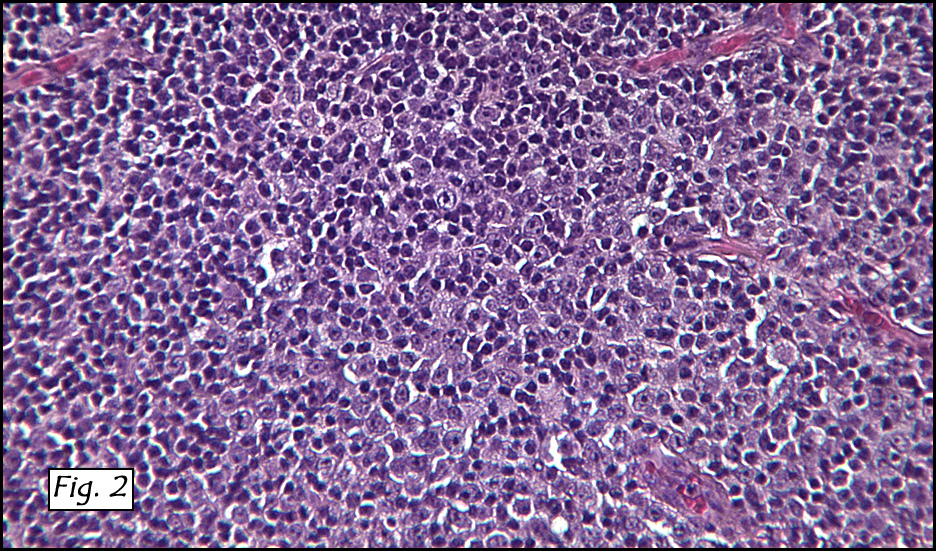
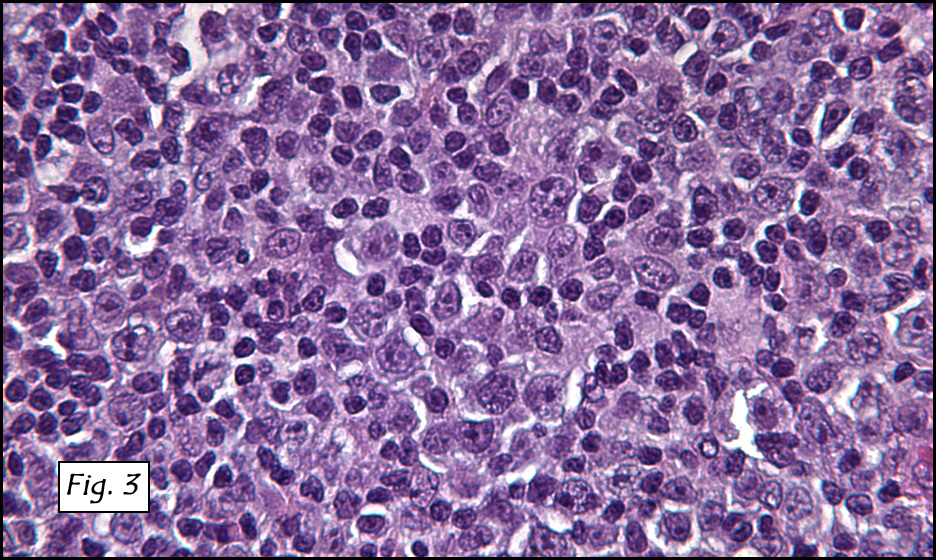
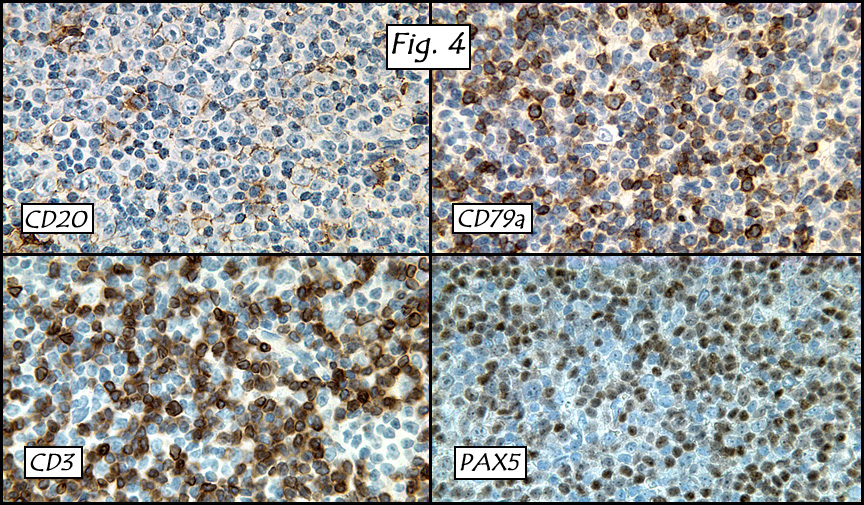
Microscopic sections revealed complete effacement of lymph node architecture by a polymorphous lymphoid infiltrate consisting of large atypical lymphoid cells with open chromatin, prominent nucleoli, and moderate amounts of cytoplasm against a background of predominately small lymphocytes (Figs. 1,2,3). Large atypical lymphoid cells were positive for CD20 and CD79a, while the smaller background lymphocytes were CD3, CD5 and PAX5 positive (Fig. 4). Epstein-Barr virus genomes were detected in the large atypical lymphoid cells by EBER in situ hybridization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “EBV positive diffuse large B-cell lymphoma of the elderlyâ€
Hannah Wong MD, Jun Wang MD, Donald Chase MD
Department of Pathology, Loma Linda University and Medical Center, Loma
Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: EBV positive diffuse large B-cell lymphoma of the elderly (EBV+ DLBCL, aka “age-related EBV-associated lymphoproliferative disorder”), is a rare B-cell lymphoproliferative disorder that occurs in elderly patients with no known history of immunodeficiency or lymphoma. The entity was first described by Oyama et al. in 2003 and was added as a distinct entity in the newly published WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues.
As the name suggests, EBV+ DLBCL of the elderly is a disease affecting patients over the age of 50 years. There is a slight male predominance of 1.4:1. Typically there is no history of immunodeficiency or lymphoma. Presentation symptoms and signs include fever, night sweats, weight loss and lymphadenopathy. Extranodal sites found at presentation include skin, lung, tonsil and stomach.
Histologically, the nodal or native tissue architecture is completely effaced by large atypical lymphoid cells/immunoblasts as well as Reed-Sternberg-like giant cells. Accompanying these elements are variable numbers of small lymphocytes, plasma cells, histiocytes, centroblasts and immunoblasts. Although EBV+ DLBCL of the elderly was originally separated into two subtypes; polymorphic lymphoproliferative disorder (PLPD) and large cell lymphoma (LCL) recent studies have shown the sub-classification to be clinically irrelevant.
The neoplastic large lymphoid cells show expression of pan-B cell markers (CD20, CD79a and PAX5), with variable expression of CD30, LMP-1 and EBNA-2. Light chain restriction may be present but has been difficult to demonstrate in most cases. CD15, CD10 and Bcl-6 are generally negative. Neoplastic cells showing EBER positivity and Ki-67 expression is generally high.
Differential diagnoses of EBV+ DLBCL of the elderly include other B-cell lymphoproliferative disorders such as Burkitt lymphoma, post-transplant lymphoproliferative disorder (PTLD), HIV-associated lymphoproliferative disorder, EBV- DLBCL, and EBV+ classical Hodgkin lymphoma (cHL). It is important to differentiate these entities in order to provide the most targeted and effective treatment for the patients.
•   Burkitt lymphoma (BL) is a highly aggressive lymphoma with three clinical variants:
- Endemic type mostly occurs in children between the ages of 4 – 7 in equatorial Africa.
- Sporadic type is more common in the United States and Western Europe, where the median age is 30 years.
- Immunodeficiency-associated BL patients are virtually all immunocompromised, mostly due to HIV infection.
BL has a variable degree of EBV involvement with endemic types having the highest association. Although the morphology of BL varies slightly in each type, the most common pattern is of medium-sized cells in a diffuse monotonous pattern with multiple benign macrophages having ingested apoptotic tumor cells resulting in the classic “starry-sky†pattern. Multiple mitotic figures may be present. Immunohistochemical stains can be helpful in differentiating BL from EBV+ DLBCL of the elderly since the malignant cells in BL are usually CD10 and BCL-6 positive while the malignant cells of EBV+ DLBCL are negative for those two markers. BL is also unique in that t(8;22) involving the c-myc oncogene is a constant feature; however this translocation has not been investigated in EBV+ DLBCL of the elderly.
•   Post-transplant lymphoproliferative disorder (PTLD) is a lymphoid proliferation that arises in immunosuppressed recipients usually involving a solid organ or bone marrow allograft. EBV has been found to be the driving force in PTLD, leading to early polyclonal proliferations and ultimately the development of lymphomas. Four morphologic categories of PTLD are:
- Early lesions resemble reactive hyperplasia and/or infectious mononucleosis. These lesions show an expanded paracortex filled with plasma cells and immunoblasts with a background of small T-cells with partial preservation of the underlying normal tissue architecture.
- Polymorphic PTLD shows effacement of the normal nodal/extranodal architecture by a mixture of large immunoblasts and plasma cells with smaller lymphocytes. Necrosis, mitoses and atypical immunoblasts may also be present.
- Monomorphic PTLD has a monomorphic infiltrate effacing nodal/extranodal tissues with confluent sheets of atypical B-cells or plasma cells.
The Hodgkin lymphoma (HL) variant is similar in morphology and immunophenotype to classical Hodgkin lymphoma. It displays Reed-Sternberg (HRS)-like cells and variants, and are positive for CD30 and CD15, but not CD20.
Despite splitting PTLD variants into four morphologies, the distinction is of limited value. The clinical history currently appears to be the most helpful criterion for differentiating PTLD from EBV+ DLBCL of the elderly.
•   HIV-related lymphomas display EBV presence about 60% of the time. They are generally aggressive B-cell lymphomas related to other lymphoproliferative disorders which are associated with HIV infection such as BL, DLBCL, primary effusion lymphoma, plasmablastic lymphoma of the oral cavity and others. Interestingly, other viruses such as Kaposi’s sarcoma-associated herpes virus/human herpes virus 8 (KSHV/HHV8) have also been found in several categories of immunodeficiency-associated lymphoma. But despite the similar morphological and immunohistochemical features of HIV- associated LPD and EBV+ DLBCL of the elderly, a positive HIV serology usually separates the two.
•   EBV+ classical Hodgkin lymphoma (cHL). Classical Hodgkin lymphoma accounts for 95% of all Hodgkin lymphomas. cHL has a bimodal age distribution with the first peak at 15 to 35 years and a second peak later in life. Approximately 30-50% of cHL have been found to be EBV positive. Patients with EBV+ cHL have a more aggressive clinical course and worse prognosis in comparison to those with EBV- cHL. Morphologically, EBV+ cHL has the classic morphology of cHL with HRS cells in a background of inflammatory cells. The large HRS cells have abundant cytoplasm and at least two large round nuclei with prominent nucleoli. These HRS cells are positive for CD30 and mostly positive for CD15 but are negative for CD45. This is in comparison to EBV+ DLBCL of the elderly which is usually positive for CD45, CD20/CD79a, variably positive for CD30 but negative for CD15. EBER has been found to be positive in the neoplastic cells of EBV+ DLBCL of the elderly more often than in the neoplastic HRS cells and their variants of EBV+ cHL. Thus, immunohistochemical studies and EBER are the most useful tools to distinguish EBV+ cHL from EBV+ DLBCL of the elderly.
•   EBV- DLBCL is virtually the same as EBV+ DLBCL of the elderly except that it may occur in patients of any age and is not EBV+. Morphologically, these two entities are virtually indistinguishable. However, EBER positivity would help separate it from the EBV+ DLBCL of the elderly.
EBV+ DLBCL of the elderly has a highly aggressive behavior; the median survival for this disease is approximately two years. Patients with EBV+ DLBCL of the elderly have been found to be less responsive to the standard chemotherapy regimens for large B-cell lymphoma compared with other forms of B-cell lymphoproliferative disorders.
Suggested reading:
1.   Nakamura S, Jaffe E.S, Swerdlow S.H.EBV+ Diffuse large B-cell of the elderly.. In: Swerdlow S.H., Campo E., Harris N.L., Jaffe E.S., Pileri S.A., Stein H., Thiele J., Vardiman J.W. (Eds.): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. IARC: Lyon, 243-244 2008.
2.   Shimoyama Y., Yamamoto K., Asano N., Oyama T., Kinoshita T., Nakamura S. Age-related Epstein-Barr virus-associated B-cell lymphoproliferative disorders: Special references in lymphomas surrounding this newly recognized clinicopathologic disease. Cancer Sci 9:1085-1091, 2008.
3.   Shimoyama Y., Oyama T., Asano Net al. Senile Epstein-barr virus-associated B-cell lymphoproliferative disorders: a mini review. J Clin Exp Hematopathol 46:1-4, 2006.
4.   Oyama T., Ichimura K., Suzuki R., et al . Senile EBV+ B-cell lymphoproliferative disorders: a clinicopathologic study of 22 patients. Am J Surg Pathol 27;16-26. 2003.
5.   Mueller S., Aigner T., Haag J., Schwartz R., Niedobitek G. Senile EBV-associated B-cell lymphoproliferative disorder of prepatellar bursa in elderly patient with multifocal urate arthropathy. Hematol Oncol 25:140-142, 2007.
6.   Oyama T., Yamamoto K., Asano N., et al . Age-related EBV-associated B-cell lymphoproliferative disorders constitute a distinct clinicopathologic group: A study of 96 patients. Clin Cancer Res 13:5124-5132, 2007.