History: A 51 year-old man with a medical history significant for hypertension, renal stones, and chronic kidney disease (with 66% function of the right kidney and 33% function of the left kidney) presented with a complex cystic mass of the left kidney. The lesion was discovered incidentally in October of 2006 and followed radiologically. The mass slowly increased in complexity and size, evolving from a radiologic Bosniak II to a Bosniak III lesion. The patient declined surgical intervention until there was a rapid, 1 cm increase in size between May and December of 2009. The patient subsequently underwent laparoscopic nephrectomy.
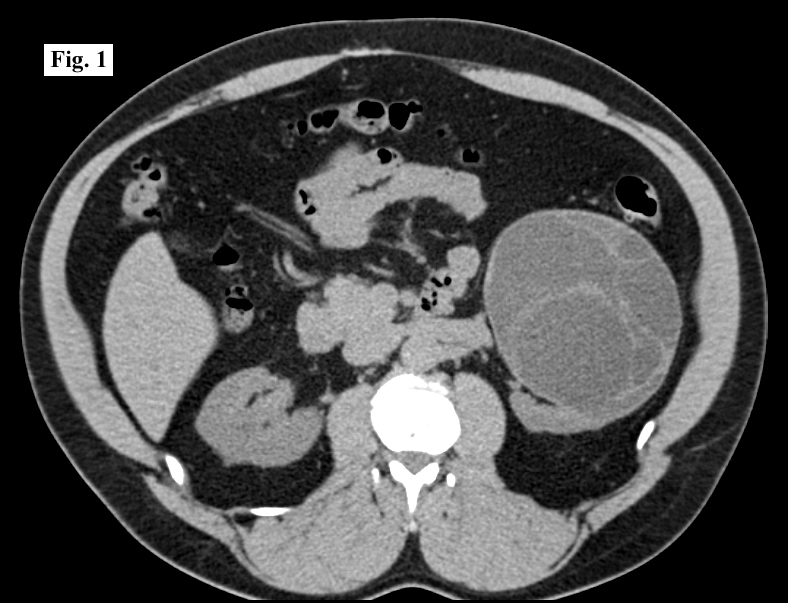
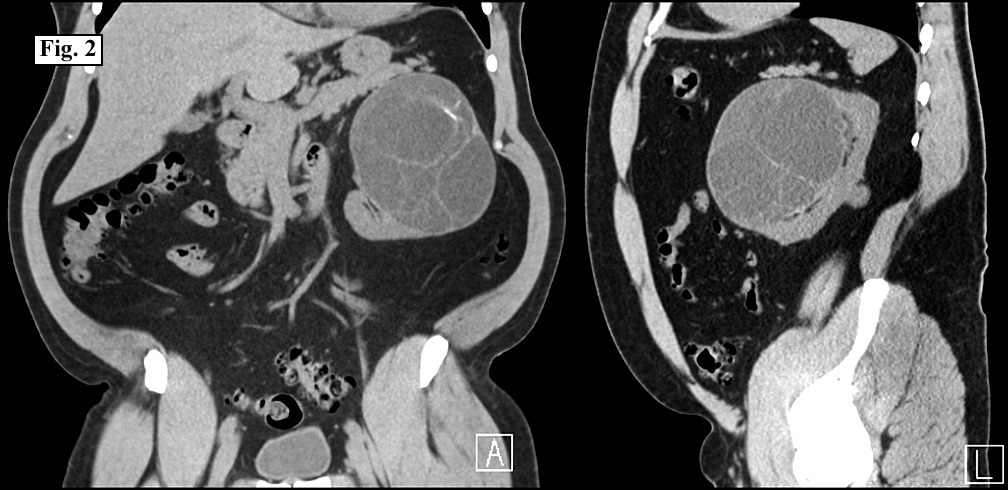
On CT scan, performed shortly before excision, the lesion measured 10.3 x 12.9 x 11.4 cm and showed multiple internal septations with mild calcifications along the upper aspect of some septations (Fig. 1, 2).
{kind=link}
{kind=link}
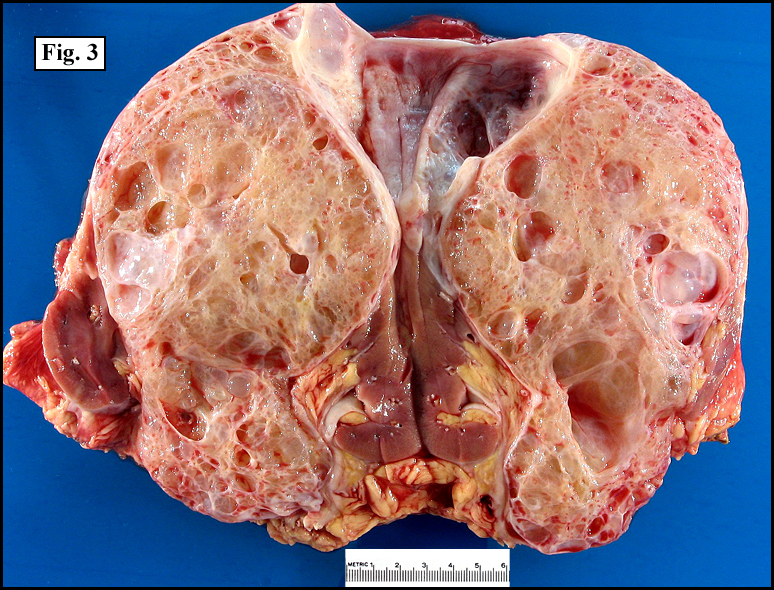
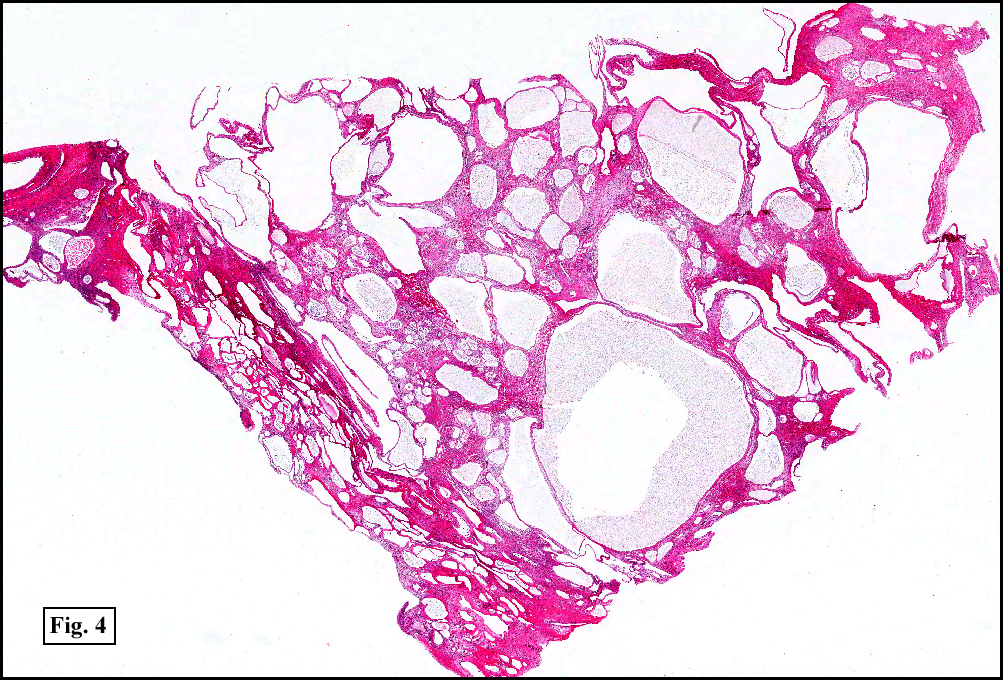
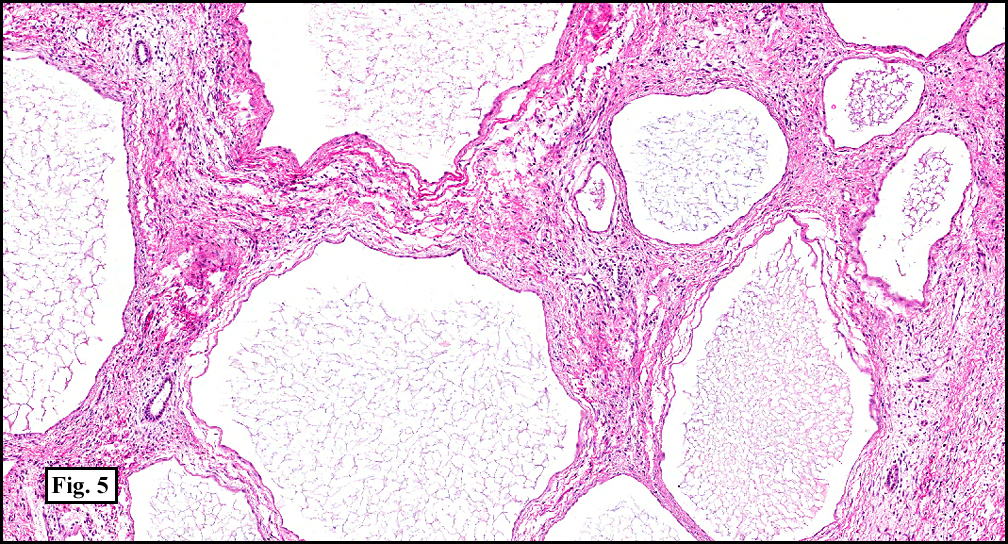
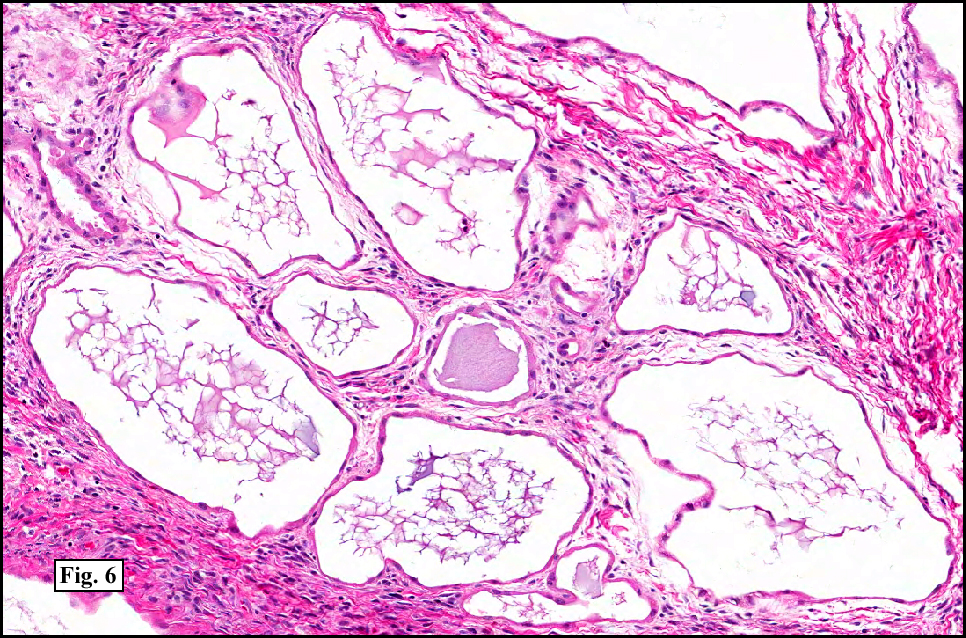
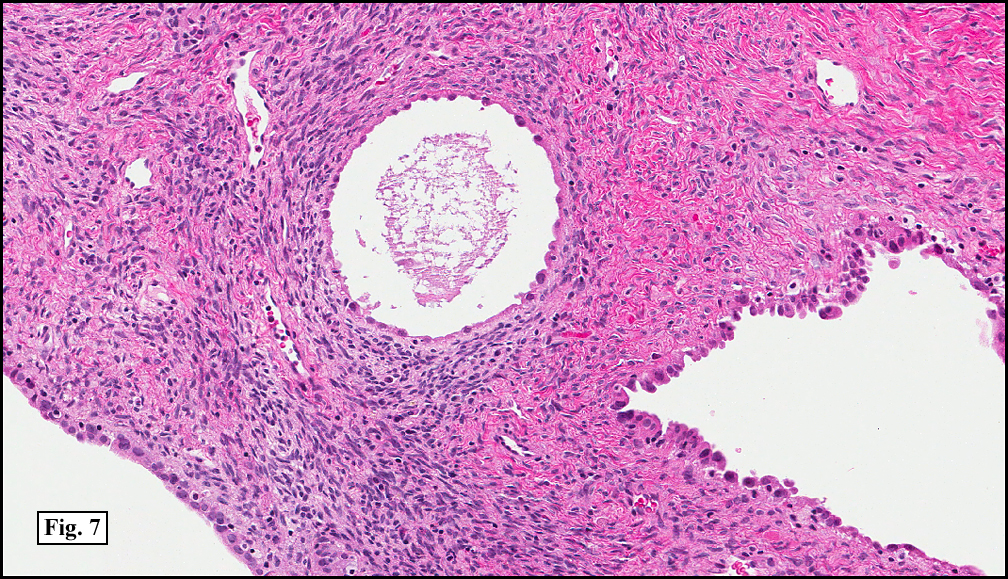
The white-tan multi-cystic mass appeared to have arisen from the mid-renal pole and pelvis (Fig. 3, gross photo from similar case). It was partially encapsulated and compressed residual normal kidney. The multiple cystic spaces were filled with transparent amber-colored fluid and delineated by smooth, thin septa (Fig. 4). The cysts were seen microscopically to be either confluent with other spaces or individual without communication (Fig. 5). The lining was by a single layer of flattened epithelium with eosinophilic cytoplasm and bland hyperchromatic nuclei (Fig. 6). Scattered regions had a hobnail morphology (Fig. 7). The fibrous elements were of dense fibrous tissue with frequent areas showing ovarian-like stroma. Rare regions had a hypocellular, myxoid morphology. The cyst walls lacked renal tubules, primitive blastema, and glomeruli.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Cystic Nephroma (CN)â€
Cassie L. Booth, MD and Donald R. Chase, MD
Department of Pathology and Human Anatomy, Loma Linda University and Medical Center, Loma Linda, CA
California Tumor Tissue Registry, Loma Linda, CA
Discussion: Cystic nephroma (CN), also known as a “multilocular renal cyst†was first described by Dr. Walter Edmunds in 1892. It is a benign process, without reported metastases and is cured by simple excision. Adult CN is to be distinguished from pediatric CN which is considered to be part of the spectrum of Wilms tumor. In adults, CNs are usually incidental findings in middle-aged women (female:male predominance of 7:1). The lesions are solitary and unilateral by definition, and typically arise from the upper pole of the kidney.
CN is usually encapsulated and although it may compress the adjacent kidney, the remaining renal parenchyma is otherwise normal. The cysts are usually non-communicating, filled with serous (or rarely hemorrhagic) fluid, and lined by a single layer of epithelial cells. This lining is usually flattened, cuboidal, or columnar, but areas of hobnail morphology are considered characteristic. Atypical cytologic features such as hyperchromasia may be seen, but are not prominent. The septa between the cysts typically consist of dense fibrous connective tissue without nephrogenic or blastemal elements. Ovarian-like stromal differentiation is also characteristic of this lesion and these areas often are immunoreactive for estrogen, progesterone, inhibin, CD10, and calretinin. Myxoid regions and scattered loose fascicles of smooth muscle may also be present.
Differential Diagnosis:
• Multilocular Cystic Renal Cell Carcinoma/Clear Cell Renal Cell Carcinoma with Prominent Cysts comprise less than 5% of clear cell RCCs. These tumors are well circumscribed with non-communicating cysts and thick fibrous septa with nodules of clear cells in some portion of the cyst wall. The lining epithelium is markedly thin or absent. Thick walls with friable material on the cyst surface and/or hemorrhage within the cyst are characteristic of carcinoma with cystic degeneration. Identification of clear cell aggregates is the hallmark in distinguishing a cystic RCC from CN (benign multilocular cysts).
• Non-neoplastic/Acquired Cystic Disease are entities which show remnants of nephrons within the septal walls and abnormal renal architecture.
• Primary Renal Synovial Sarcoma consists of monomorphic, plump spindle cells frequently interspersed with large cysts. The cysts are lined by bland, mitotically inactive epithelial cells. The spindle cells are immunoreactive for EMA, CD56, and sometimes CD99 but never ER (which is frequently expressed by the ovarian-like stroma of CNs). The tumor is also characterized cytogenetically by translocation t(X;18)(p11.2/q11.2) resulting in a distinctive SYT-SSX fusion gene.
• Tubulocystic carcinoma has only recently been described and did not appear in the 2004 WHO classification. It has a distinctive gross appearance usually of a spongy off-white cut surface composed of clear fluid-filled cysts which appear to be uniform in size. But microscopically the cysts show considerably size variation, some as small as a renal tubule. The cysts are separated by thin fibrous septa and are lined by a single layer flattened, cuboidal, or hobnail carcinoma cells with spherical nuclei and prominent nucleoli. Necrosis is rare and mitotic figures are infrequently encountered.
• Mixed Epithelial and Stromal Tumor (MEST) is perhaps the most controversial differential for CN, as there are many striking similarities in their clinical behavior, morphologic features, and immunohistochemical properties. Both are benign, biphasic tumors with epithelial and stromal components typically arising in middle-aged/peri-menopausal women. MESTs are well-circumscribed but lack a thick fibrous capsule, however compressed renal tissue may form a pseudocapsule. Unlike CNs which are diffusely cystic, MESTs are composed of cystic and solid areas and the septa between the cysts are typically thicker than that of CNs. The larger cysts may be lined by cuboidal or columnar epithelium with occasional papillary tufts while the smaller cyst linings resemble that of CNs. Like CNs, the stroma consists of a variably cellular spindle cell population ranging from myxoid-like areas to cellular, mesenchymal ovarian-stroma like tissue. These ovarian-stroma like regions are typically more pronounced in MESTs and more frequently immunoreactive for estrogen and progesterone. Recent publications also indicate that MESTs and CNs have similar molecular characteristics. Although these entities are classified separately in the most recent edition of the WHO (2004), there is evidence that they may in fact be opposite ends of a morphologic spectrum for a single neoplasm and the term renal epithelial and stromal tumor (REST) has been proposed as a unifying term.
Suggested Readings:
1. Antic T, Perry KT, Harrison K, et al. Mixed Epithelial and Stromal Tumor of the Kidney and Cystic Nephroma Share Overlapping Features: Reappraisal of 15 Lesions. Arch Pathol Lab Med. 130:80-85, 2006.
2. Eble JN SG, Epstein JI, Sesterhann IA. Classification of Tumours. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. Lyon, France: IARC Press; 2004.
3. Moch H. Cystic Renal tumors: New Entities and Novel Concepts. Adv Anat Pathol 12(3):209-214, 2010.
4. Mohanty SK, Parwani AV. Mixed Epithelial and Stromal Tumors of the Kidney: An Overview. Arch Pathol Lab Med 133:1483-1486, 2009.
5. Murphy WM, Grignon DJ, Perlman EJ. Tumors of the Kidney, Bladder, and Related Urinary Structures. Washington, DC: Armed Forces Institute of Pathology; 2004.
6. Turbiner J, Amin M, Humphrey PA, et al. Cystic Nephroma and Mixed Epithelial and Stromal Tumor of Kidney: A Detailed Clinicopathologic Analysis of 34 Cases and Proposal for Renal Epithelial and Stromal Tumor (REST) as a Unifying Term. Am J Surg Pathol 31(4):489-500, 2007.