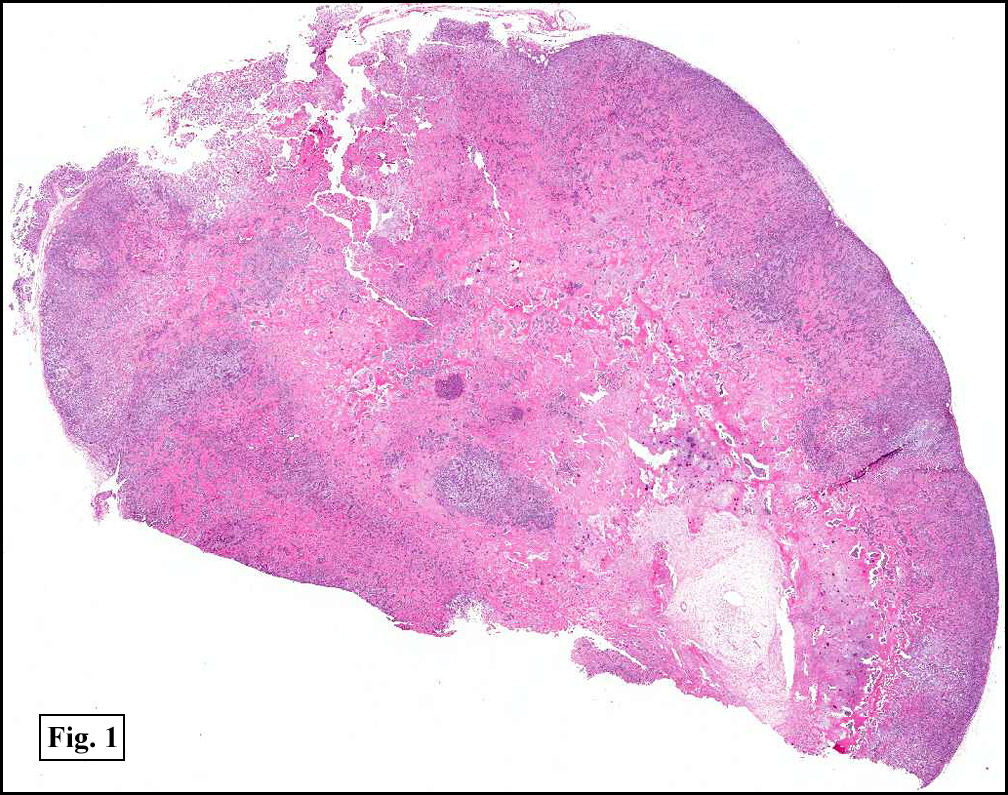
History: A 48-year-old man noticed an enlarging, freely moveable mass in the left shoulder. The excised specimen consisted of two portions of firm lobulated tan tissue each approximating 2.0 cm in greatest diameter.
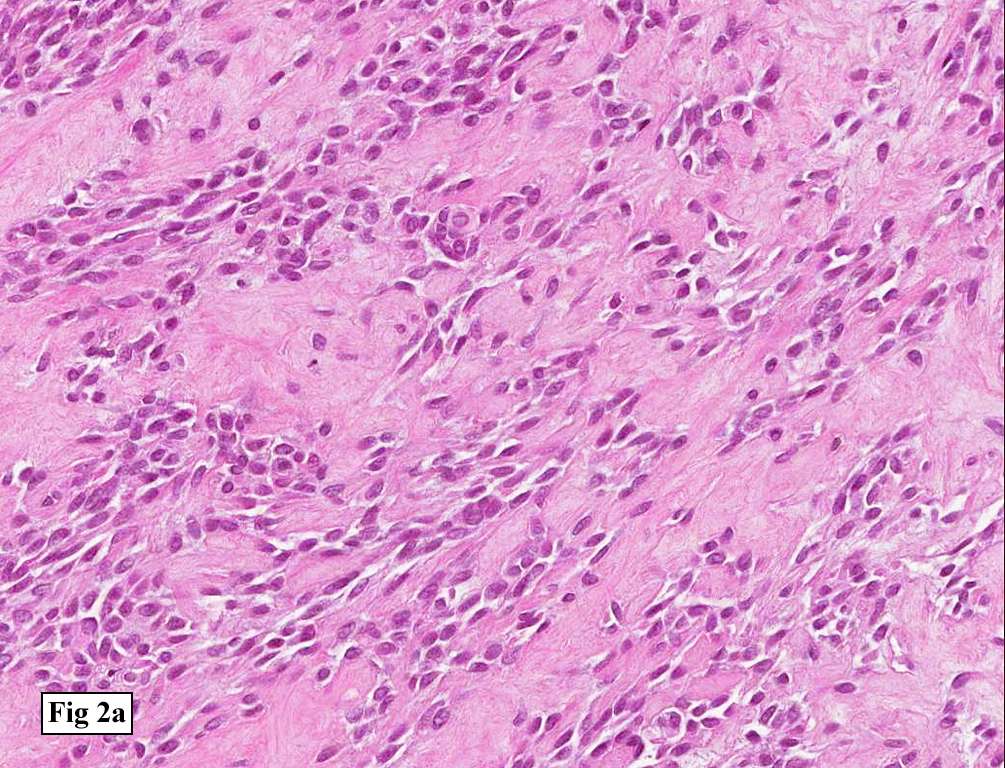
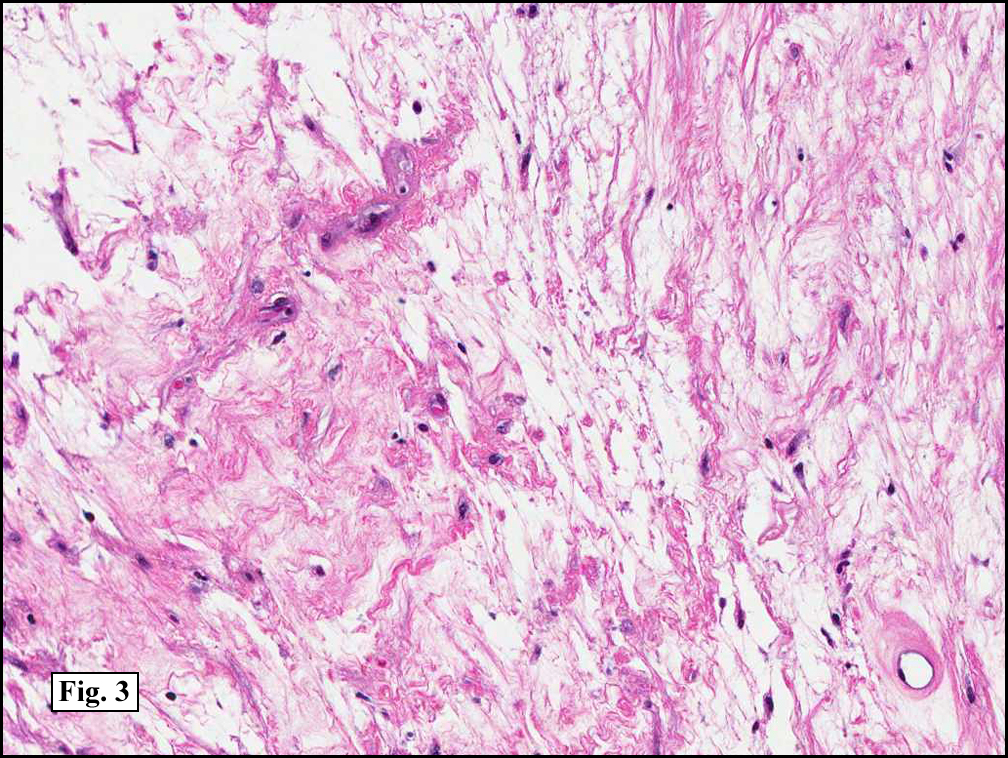
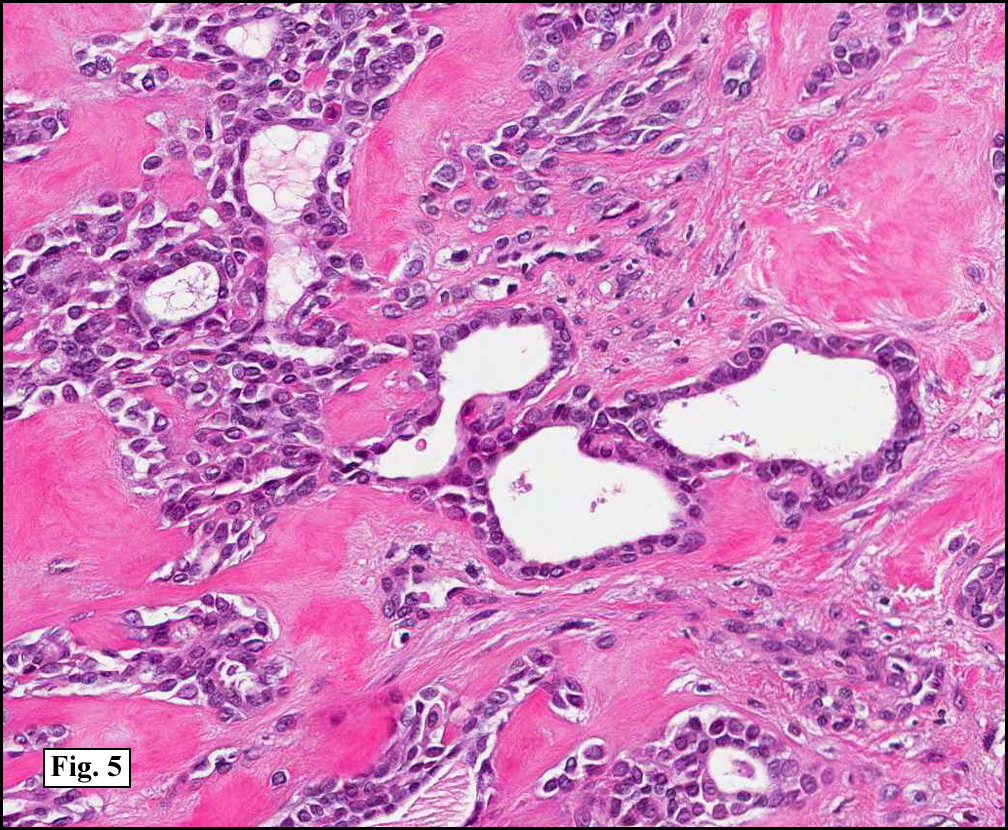
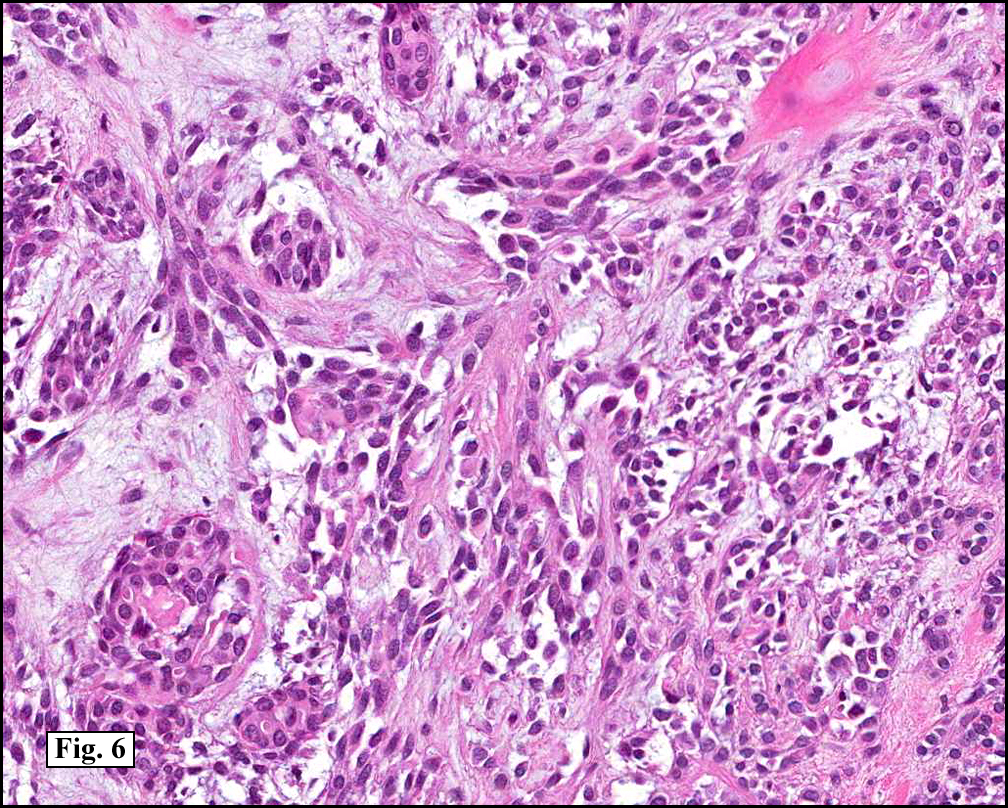
The tumor was well-circumbscribed and varied in cellularity (Fig. 1). It microscopically had an eosinophilic stroma consisting of spindled and fibrous cells (Fig. 2a, 2b), myxoid regions (Fig. 3) and chondroid areas (Fig. 4). Clusters and solid sheets of cell-enveloped ducts generally had two layers of cuboidal cells (Fig. 5). There were scattered mitotic figures and mild pleomorphism (Fig. 6). Calcifications and ossification were also present. Immunohistochemical stains for CEA, CK, vimentin and S100 (not shown) were positive.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Chondroid Syringomaâ€
Jonathan Zumwalt, MSIV, and Donald R. Chase, MD
Department of Pathology and Human Anatomy, Loma Linda University and
Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: First described by Billroth in 1859 as “mixed tumor of the skin†the term “chondroid syringoma†(CS) was first used by Hirsch and Helwig in 1961 to describe the same entity which had also been known as mixed tumor, eccrine syringoma, cutaneous mixed tumor, and pleomorphic adenoma of the skin. The lesions also have more recently been sub-classified as apocrine or eccrine, or as a combination “mixedâ€. The tumor typically presents in mid to late-aged men as a solitary, slowly growing nodule on the head or neck. However, it may occur in either gender, in any skin site, in most any age (range 10-96). It is usually between 0.5-3.0 cm in diameter.
The apocrine mixed tumors are generally well-defined tumors with a background of fibrous, myxoid and/or chondroid stroma. Although most tumors show a mixture of all three elements, it is not uncommon for only two to be present. The stromal areas may contain calcifications or areas of ossification.
The glandular portion of the tumor shows ducts lined by two layers of cuboidal epithelium. Some of the ducts are variably dilated and may have keratinous cysts. Eosinophilic globules composed of collagen (collagenous spherulosis) may be found in both the lumina of the glandular elements and in the stroma. Metaplastic squamous changes may also be present.
The cells of this tumor usually express CEA and CK, while the cells in the outer layer of the tubular structures contain vimentin and S100. The presence of CEA and CK suggest apocrine origin of the intrafollicular ducts. Type IV collagen, tenacin, and fibronectin, are usually found in the mucoid-like or chondroid stroma. Type II collagen is generally found in both the stromal and epithelial compartments; otherwise it is only expressed in cartilage.
A rare variant of CS is the so-called “hyaline cell-rich chondroid syringoma”. This unique tumor is composed of epithelial cells with eosinophilic hyaline that displaces the nucleus and results in a plasmacytoid appearance. Although these tumors may be mistaken for plasmacytomas, they usually show duct formation.
The eccrine mixed CS differs from the apocrine variant in having numerous small syringoma-like ducts within a cartilaginous and myxoid stroma. These ducts express both CEA and CK.
The malignant variant of the CS is quite uncommon, and is initially indolent for months or years and abruptly shows rapid growth. It mostly occurs in women (2:1) usually in the extremities or trunk. The tumor is generally larger than the benign variant (2-3 cm). Microscopic examination shows persistence of the lobules, and infiltration/invasion of the adjacent tissue. Cords of cells with cuboidal or polygonal shapes with glandular differentiation are characteristic. The malignant variant often shows pleomorphism, mitotic figures and invasion into lymphatics. The tumor cells express CK and the cells lining the lumens are CEA positive. Approximately 30-40% metastasize.
Suggested Reading:
A special thanks to Martin Mihm and his 120th CTTR Semi-Annual Pathology Slide Seminar Handout.
Barnett MD, Wallack MK, Zuretti A, Mesia L, Emery RS, Berson AM. Recurrent malignant chondroid syringoma of the foot: a case report and review of the literature. Am J Clin Oncol. 2000 Jun;23(3):227-32.
Bhargava D, Bhusnurmath S, Daar AS. Chondroid syringoma of the nose: report of a case. J Laryngol Otol. 1997 Sep;111(9):862-4.
Kazakov DV, Belousova IE, Bisceglia M, Calonje E, Emberger M, Grayson W, Hantschke M, Kempf W, Kutzner H, Michal M, Spagnolo DV, Virolainen S, Zelger B. Apocrine mixed tumor of the skin (“mixed tumor of the folliculosebaceous-apocrine complex”). Spectrum of differentiations and metaplastic changes in the epithelial, myoepithelial, and stromal components based on a histopathologic study of 244 cases. J Am Acad Dermatol. 2007 Sep;57(3):467-83.
Metzler G, Schaumburg-Lever G, Hornstein O, Rassner G. Malignant chondroid syringoma: immunohistopathology. Am J Dermatopathol. 1996 Feb;18(1):83-9.
Sungur N, Uysal A, Gümüş M, Koçer U. An unusual chondroid syringoma. Dermatol Surg. 2003 Sep;29(9):977-9.
Yavuzer R, BaÅŸterzi Y, Sari A, Bir F, Sezer C. Chondroid syringoma: a diagnosis more frequent than expected. Dermatol Surg. 2003 Feb;29(2):179-81.
Yim YM, Yoon JW, Seo JW, Kwon H, Jung SN. Pleomorphic adenoma in the auricle. J Craniofac Surg. 2009 May;20(3):951-2.