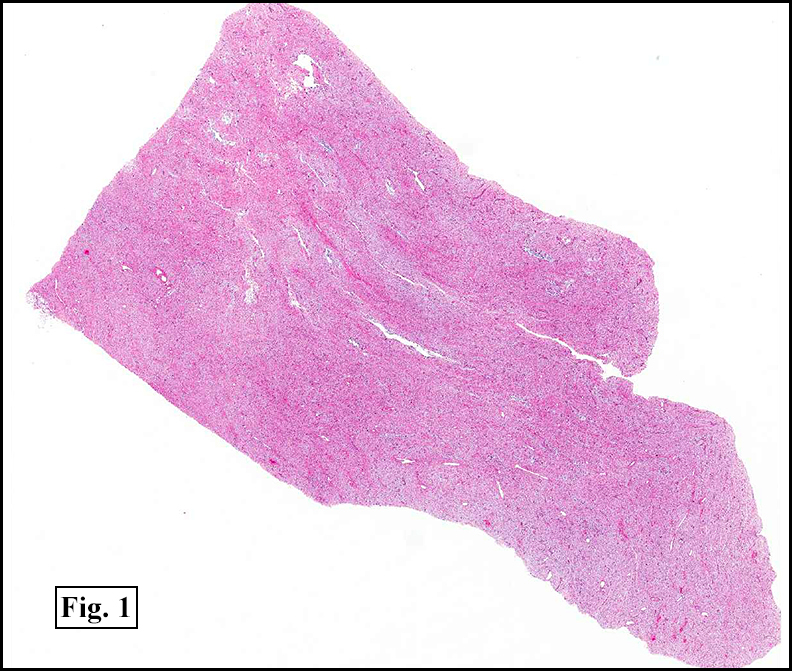
History: A 13-month-old male infant underwent surgical resection of a 6.0 x 5.6 x 2.0 cm subxiphoid body wall mass. The cut surface was soft and homogenously gray-tan.
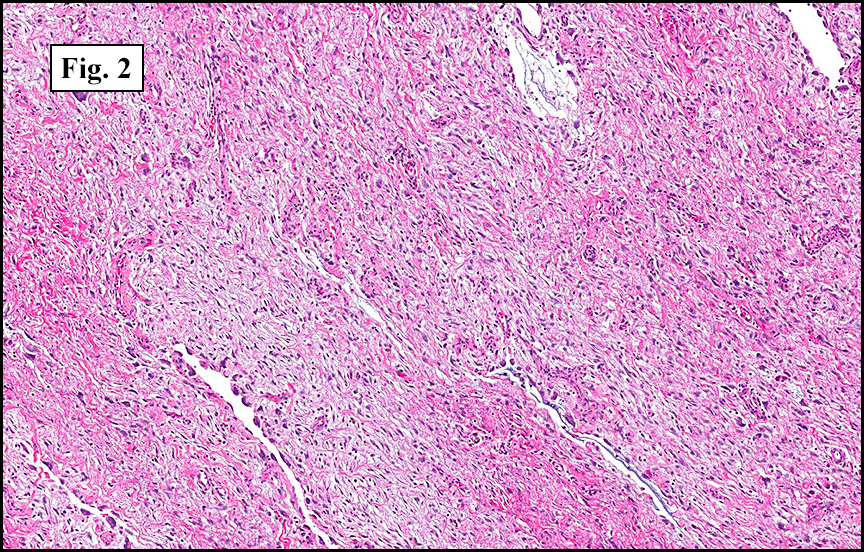
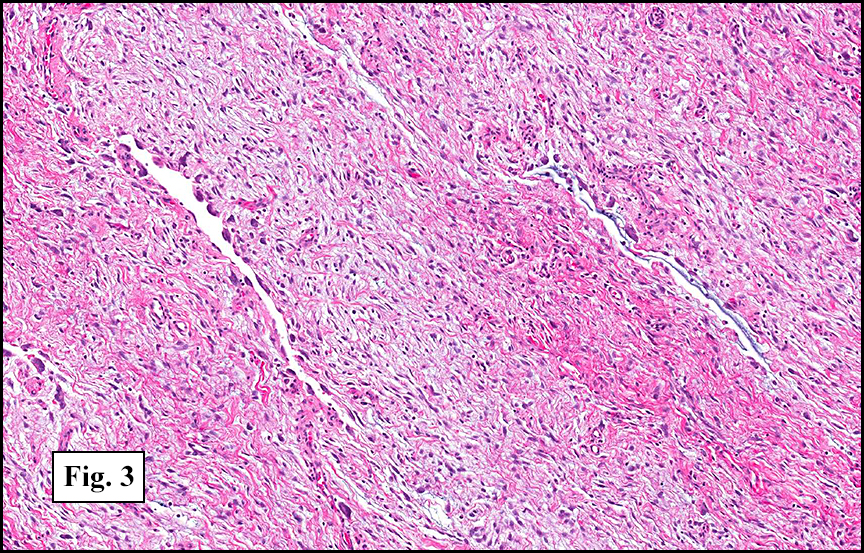
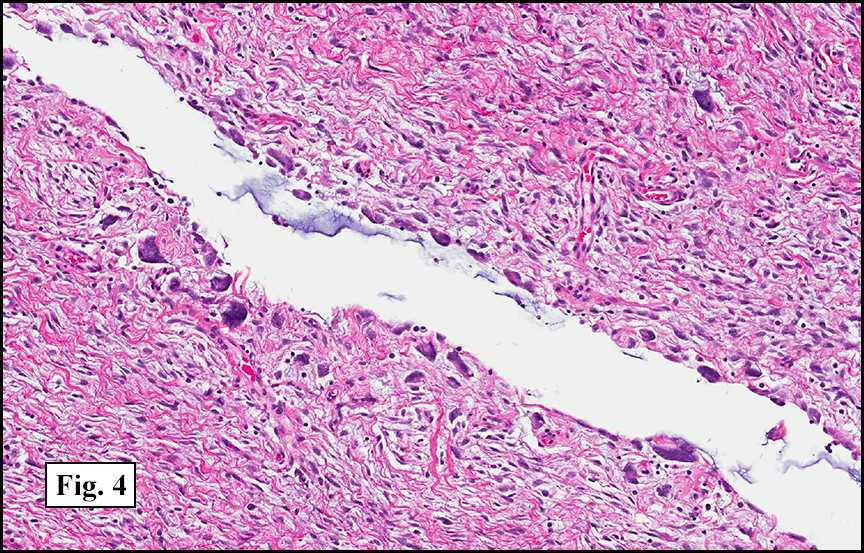
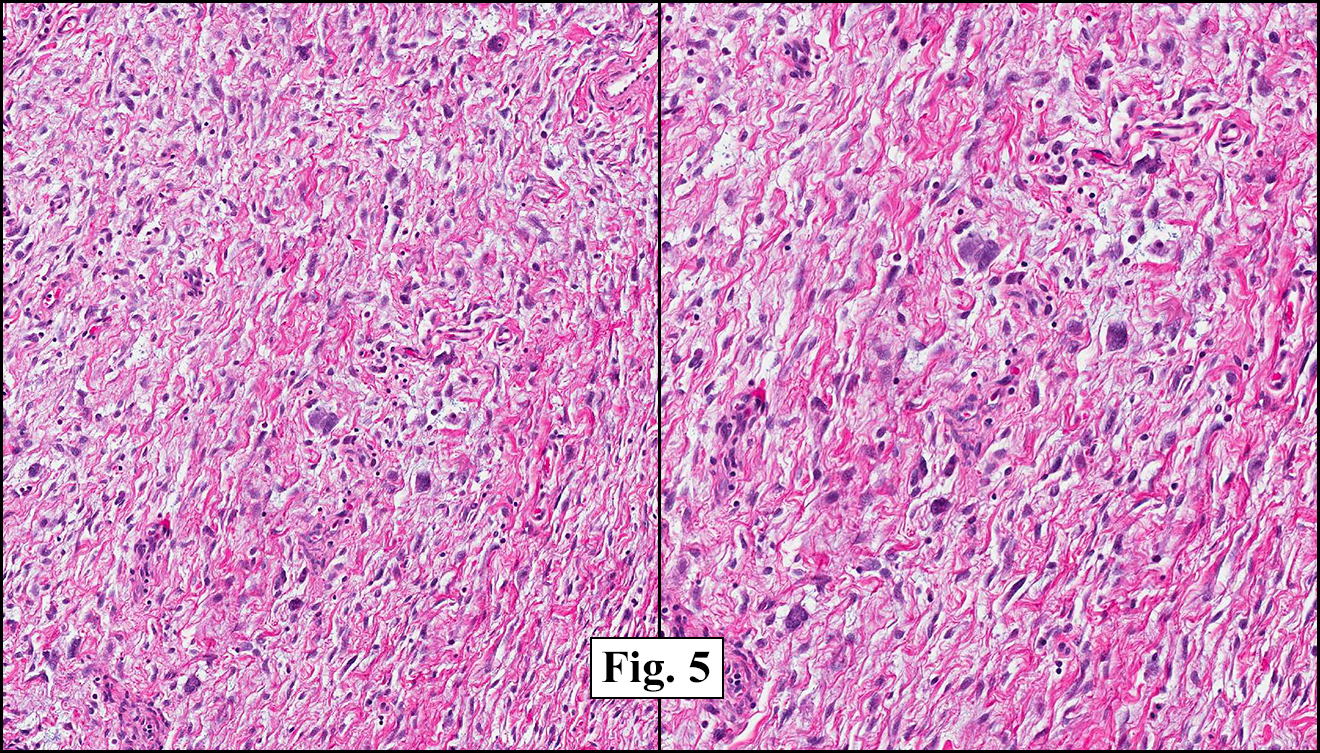
The stroma was loosely arranged and consisted of undulating spindle cells (Fig. 1, 2) intermixed with irregularly shaped “pseudovascular†spaces (Fig. 3). Discontinuous rows of hyperchromatic giant cells lined the peripheries of these spaces (Fig. 4). Giant cells and multinucleated-appearing cells were scattered throughout the stroma (Fig. 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Giant Cell Fibroblastoma, Chest Wallâ€
Matthew S. Johnson, PSF, and Donald R. Chase, MD
Department of Pathology and Human Anatomy
California Tumor Tissue Registry
Loma Linda University and Medical Center, Loma Linda, California
Discussion: Initially described by Shmookler and Enzinger in 1982, giant cell fibroblastoma (GCF) is classified as a fibrohistiocytic tumor commonly felt to be the juvenile form of dermatofibrosarcoma protuberans (DFSP). It is usually diagnosed in infancy or childhood, with two-thirds being discovered by 5 years of age and about 90% by 10 years (median diagnostic age is 3 years). Rare cases have been reported in adults. GCF usually affects males and typically presents as a painless mass in the abdominal wall, groin, or back. Grossly, they are poorly circumscribed and gelatinous. The cut surface is usually gray to yellow.
Histologically, GCFs are variably cellular and composed of spindle and stellate cells within a collagenous, sometimes myxoid stroma. The nuclei are small and uniform without significant numbers of nucleoli. Scattered throughout the stroma are hyperchromatic giant cells with large vesicular nuclei, often with prominent nucleoli. Occasionally the giant cells appear multinucleated; however, ultrastructural examination suggests that most actually have a single, multilobated nucleus. The defining feature of this tumor is the intervening, large, irregular pseudovascular spaces that are partially lined by the giant cells. No endothelial lining is present.
Immunohistochemical studies show the tumor stroma and pseudovascular lining to be negative for S-100, cytokeratin, desmin, and CD31. CD34 is typically weakly positive in the stromal elements.
GCF appears to be closely related to DFSP. Cases of GCF recurring as DFSP (and vice versa) have been documented, and some tumors show both neoplasms. Cytogenetic analysis has revealed the presence of a (17:22) translocation in both phenotypes. Evidence suggests that a linear arrangement of this abnormality occurs in GCF while a ring form takes place in DFSP.
Differential Diagnosis:
• Myxoid liposarcoma may resemble GCF with myxoid stroma; however, the tendency to occur in deep tissues, the presence of lipoblasts, a delicate vasculature, and lack of giant cells separates it from GCF.
• Myxoid malignant fibrous histiocytoma (myxofibrosarcoma) may have histologically similar stroma and can have large cells demonstrating pleomorphism and multinucleation. A vascular network and mitotic activity differentiates it from GCF, as does a lack of space-lining pleomorphic cells.
• Angiosarcomas demonstrate irregular branching vascular channels that are lined by multiple layers of cells with large hyperchromatic nuclei. These lesions are distinguished from GCF by their high mitotic activity, atypical nuclei of the vascular lining cells, and expression of CD31.
• Lymphangiomas contain angiectatic spaces, but these spaces are often surrounded by a layer of smooth muscle, and not by pleomorphic cells. Lymphoid aggregates may also be present in the surrounding stroma.
About 50% of GCF cases recur. Recurrences are not aggressive and metastatic disease has not been reported. Treatment of choice is wide local excision; however, less invasive therapy with routine follow-up is also a consideration.
Suggested Reading:
Terrier-Lacombe MJ; Guillou L; Maire G; Terrier P; Vince DR; de Saint Aubain Somerhausen N; Collin F; Pedeutour F; Coindre JM. Dermatofibrosarcoma protuberans, giant cell fibroblastoma, and hybrid lesions in children: clinicopathologic comparative analysis of 28 cases with molecular data – a study from the French Federation of Cancer Centers Sarcoma Group. Am J Surg Pathol 2003 Jan;27(1): p27-39.
Sandberg AA; Bridge JA. Updates on the cytogenetics and molecular genetics of bone and soft tissue tumors. Dermatofibrosarcoma protuberans and giant cell fibroblastoma. Cancer Genet Cytogenet 2003 Jan 1;140(1): p1-12.
Pascual A; Sanchez-Martinez C; Moreno C; Burdaspal-Moratilla A; Lopez-Rodriguez MJ; Rios L. Dermatofibrosarcoma protuberans with areas of giant cell fibroblastoma in the vulva: a case report. Eur J Gynaecol Oncol 2010;31(6): p685-9.
Najarian DJ; Morrison C; Sait SN; Meguerditchian AN; Kane J; Cheney R; Zeitouni NC. Recurrent giant cell fibroblastoma treated with Mohs micrographic surgery. Dermatol Surg 2010 Mar;36(3): p417-21.
Layfield LJ; Gopez EV. Fine-needle aspiration cytology of giant cell fibroblastoma: case report and review of the literature. Diagn Cytopathol 2002 Jun;26(6): p398-403.
Aliagaoglu C; Bakan V; Atasoy M; Sahin O; Toker S; Albayrak M. A very large, rapidly developing, congenital giant cell fibroblastoma in a 5-month old infant. J Dermatol 2006 Mar;33(3): p182-6.