History: An 85-year-old woman presented with pelvic discomfort of unknown duration. She had undergone a hysterectomy in the remote past. Physical examination revealed a pelvic hernia, with loops of bowel protruding through the introitus.
The subsequent surgery found an unexpected 245 gram, 9.0 x 3.0 x 0.4 cm mass in the right ischiorectal fossa. It was covered with gray-white mucosa that was glistening, gelatinous, and gray-white to gray-yellow.
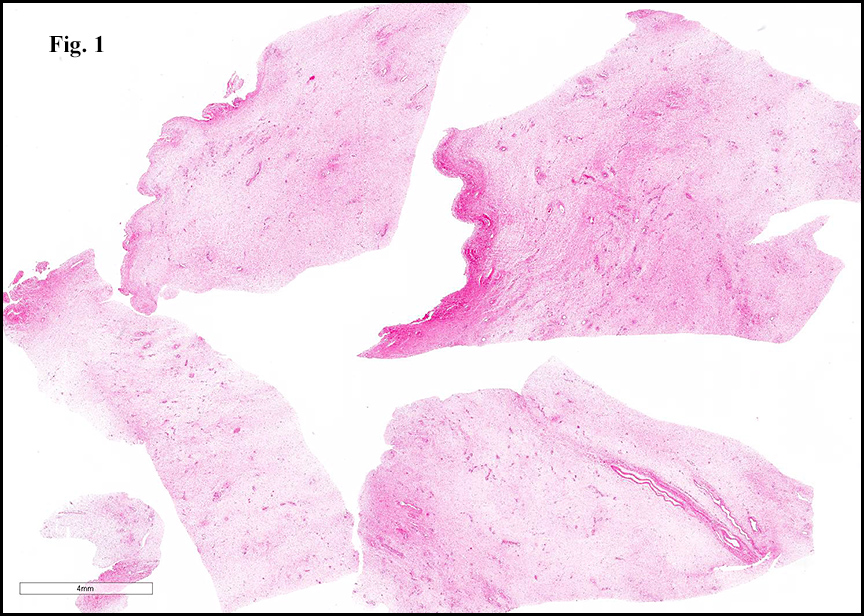
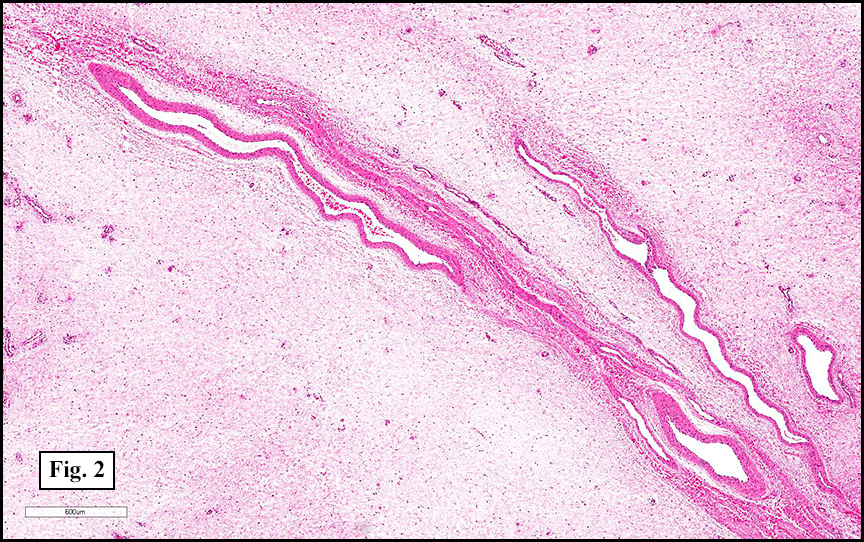
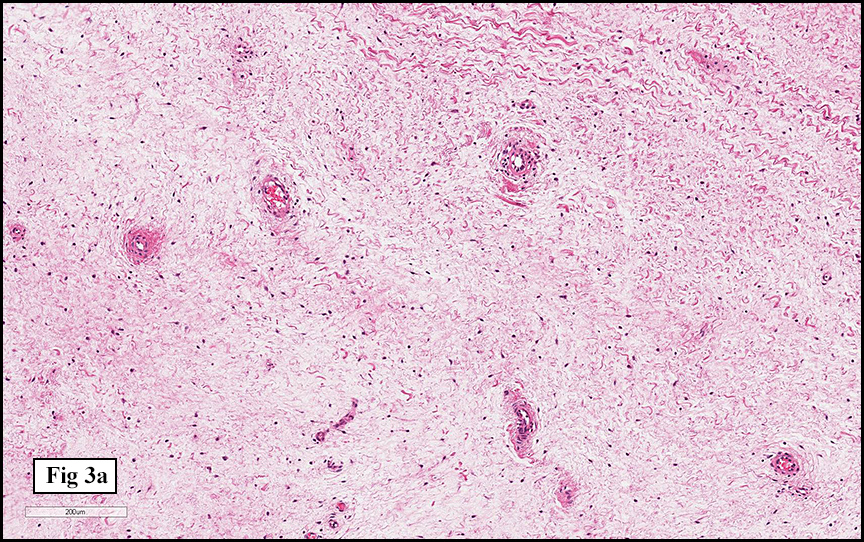
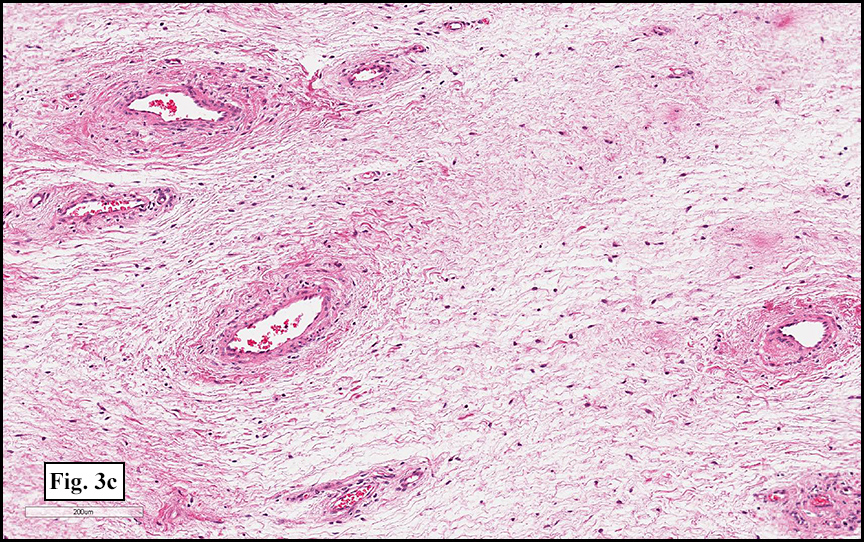
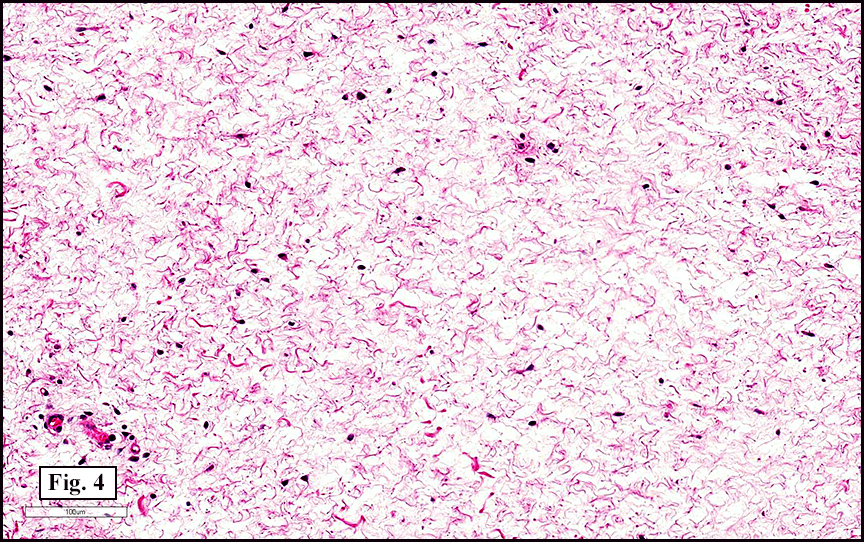
Microscopically, the tumor was hypocellular, comprised of uniform spindle cells evenly distributed in an abundant myxoid stroma (Fig. 1). Within the myxoid stroma were numerous medium to large, thick-walled, occasionally hyalinized vessels (Fig. 2, 3a, 3b, 3c). Adjacent to some of the vessels were clusters of loose fibrillary collagen and mucin (Fig. 4). The tumor showed no significant pleomorphism, mitotic activity, nor necrosis. Immunohistochemical stains were positive for vimentin, and negative for desmin (except normal positivity in vessel walls).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Aggressive Angiomyxoma, Pelvis
Elif L. Akin, M.D. and Donald R. Chase, M.D.
Department of Pathology & Human Anatomy
Loma Linda University Medical Center, Loma Linda, California
Discussion: Aggressive angiomyxoma (AAM) is a rare mesenchymal neoplasm originally described in 1983 by Steeper and Rosai. Their study of nine female patients described the tumor as a benign-appearing myxoid gynecologic neoplasm with prominent vascular features. In sharp contrast to conventional myxomas, which have a similar myxoid stroma, this new entity was distinctive with its increased vascularity and propensity for local invasion and frequent recurrence.
While AAM has now been described in patients ranging from 6 to 77 years of age, most reported cases tend to occur in reproductive-age women during their third and fourth decades. With a female to male ratio of about 6:1, this tumor generally arises in the vulva, vagina, pelvis, and perineum. In males, AAM occurs in analogous anatomic sites, including inguinal-scrotal and perineal regions.
Patients usually present with an asymptomatic perineal or vulvar mass that is discovered on routine physical exam or radiographic imaging. Symptoms, when present, are typically related to the tumor’s mass effect, which may result in the displacement of other viscera (e.g., bowel, bladder, etc.). Clinically, these tumors have been mistaken for labial cysts including Gartner and Bartholin cysts.
Grossly, aggressive angiomyxomas are usually large, often greater than 10 cm. Of note, Steeper and Rosai described one tumor measuring 60 cm in greatest dimension and mentioned another that reportedly weighed over five kilograms! AAMs generally have a smooth, unencapsulated outer surface and a soft, lobulated, gelatinous blue-gray cut surface with focal areas of hemorrhage.
Microscopically, AAM is characterized by a bland, hypocellular myxoid stroma with uniformly distributed fibroblasts and myofibroblasts. Vessels are prominent, variably sized, and usually show thick muscular walls with occasional hyalinization. Extravasated red blood cells are often seen. While the tumor may entrap soft tissue elements, significant nuclear pleomorphism, mitotic activity, and necrosis are not typically present. Immunohistochemical stains reveal diffuse positivity for vimentin and desmin. AAM may also show reactivity for estrogen receptors, progesterone receptors, smooth muscle actin and muscle-specific actin. Staining for S100 is typically negative but may highlight entrapped neural elements.
At this time, wide local excision is the mainstay therapy for AAM. Despite a bland microscopic appearance, AAM has an infiltrative growth pattern and lacks a well-defined capsule. Complete surgical excision is therefore difficult and many of the tumors are incompletely excised. Local recurrence rates approximate 30%. Although this neoplasm has historically been regarded as benign, there have been two documented cases of metastatic aggressive angiomyxoma (to the lung and mediastinum). Recent studies indicate that there may be a role for gonadotropin-releasing hormone agonists as neoadjuvant therapy. Indeed, these tumors are usually positive for estrogen and progesterone receptors, suggesting that there may be a hormonal influence on tumorigenesis. While surgery remains the main therapy for aggressive angiomyxoma, further exploration of hormonal therapy shows promise.
The differential diagnosis for aggressive angiomyxoma includes a broad spectrum of mesenchymal entities ranging from benign to aggressive neoplasms.
• Angiomyofibroblastoma: Although this benign genital stromal tumor occurs in a similar location and shares some histologic features with aggressive angiomyxoma, most angiomyofibroblastomas are small (usually < 3 cm), well-circumscribed neoplasms that generally do not have myxoid features. In contrast to the muscular, thick-walled vessels of aggressive angiomyxoma, the vasculature in angiomyofibroblastoma is often thin-walled, hyalinized, and surrounded by epithelioid cells, imparting an appearance of perivascular hypercellularity. Additionally, multinucleated giant cells are frequently identified in angiomyofibroblastomas. Distinguishing these tumors is important because, unlike aggressive angiomyxoma, angiomyofibroblastoma rarely recurs after excision. • Cutaneous myxoma (superficial angiomyxoma): This neoplasm, like aggressive angiomyxoma, is characterized by a hypocellular, myxoid stroma with evenly-spaced stellate or spindled cells. Although cutaneous myxoma may also demonstrate prominent vasculature, in contradistinction to AAM, cutaneous myxoma has thin-walled, arborizing vessels, a predilection for more superficial locations (usually dermal or subcutaneous), and characteristic stromal inflammation with increased numbers of neutrophils. • Myxoid leiomyoma: While this tumor can also be large and occur in the pelvic region, it lacks the vascularity of an aggressive angiomyxoma. Furthermore, the smooth muscle cells in a myxoid leiomyoma tend to be arranged in a loosely fascicular pattern, are larger, and have more eosinophilic cytoplasm than the cells of an aggressive angiomyxoma. • Myxoid neurofibroma: This lesion may be distinguished from aggressive angiomyxoma by its wavy or “buckled†nuclei, lack of prominent vasculature, and diffuse S100 positivity. • Pelvic fibromatosis: Though this infiltrative condition also occurs in reproductive-age women and may demonstrate prominent areas of myxoid change, pelvic fibromatosis does not have large, thick-walled vessels and is generally characterized by a spindle cells and collagen bundles in a fascicular arrangement. In summary, aggressive angiomyxoma is a large, infiltrative tumor that typically occurs in the pelvic and vaginal areas of reproductive-age females. It is comprised of spindled and stellate cells that are uniformly distributed in a myxoid stroma, which demonstrates thick-walled and hyalinized vessels. While this tumor appears to be cytologically bland, appropriate identification is important to warrant aggressive surgical intervention to prevent local recurrence. Suggested reading:
Kurman RJ. Blaustein’s Pathology of the Female Genital Tract: 4th ed. Springer-Verlag: New York. 1994: 114-115.
Blandamura S, Cruz J, Faure Vergara L, et al. Aggressive angiomyxoma: a second case of metastasis with patient’s death. Hum Pathol. 2003; 34: 1072-1074.
Fletcher CD. Diagnostic Histopathology of Tumors 3rd ed. Churchill Livingstone Elsevier. 2007: 742-743.
Robboy SJ, Mutter GL, Prat J, et al. Robboy’s Pathology of the Female Genital Tract: 2nd ed. Churchill Livingstone Elsevier. 2008: 103-105.
Sereda D, Sauthier P, Hadjeres R, Funaro D. Aggressive Angiomyxoma of the Vulva: A Case Report and Review of the Literature. J Lower Gen Tract Disease 2009: 46-50.
Siassi RM, Papadopoulos T, Matzel KE. Metastasizing Aggressive Angiomyxoma. N Engl J Med. 1999; 341 (23): 1772.
Skalova A, Michal M, Husek K, et al. Aggressive Angiomyxoma of the Pelvioperineal Region: Immunohistological and Ultrastructural Study of Seven Cases. Am J Dermatopathol. 1993; 15: 446-451.
Steeper TA, Rosai J. Aggressive Angiomyxoma of the Female Pelvis and Perineum: Report of Nine Cases of a Distinctive Type of Gynecologic Soft-Tissue Neoplasm. Am J Surg Pathol. 1983; 7: 463-475.
Sutton BJ, Laudadio J. Aggressive Angiomyxoma. Arch Pathol Lab Med. 2012; 136 (2): 217-221.
Weiss S, Goldblum J. Enzinger & Weiss’s Soft Tissue Tumors: 5th ed. Mosby/Elsevier Inc: Philadelphia. 2008: 1081-1088.