History: A 3 year old girl presented with a solitary, painless, rapidly growing shoulder mass. On physical exam it was mobile, non-tender and irregular. The overlying skin did not show any changes. Neither the patient nor her family had any pertinent past medical history. The excised specimen was 5.5 x 5.0 x 3.0 cm, tan-yellow, poorly circumscribed and predominantly comprised of fibrofatty tissue.
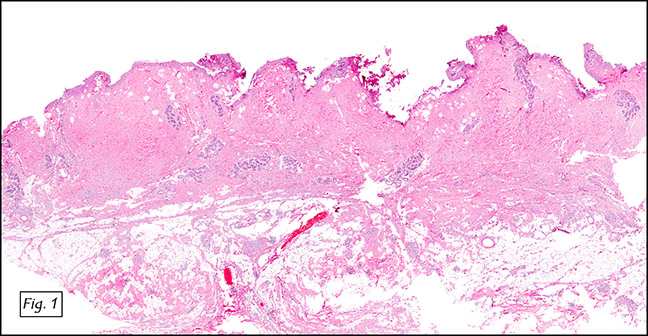
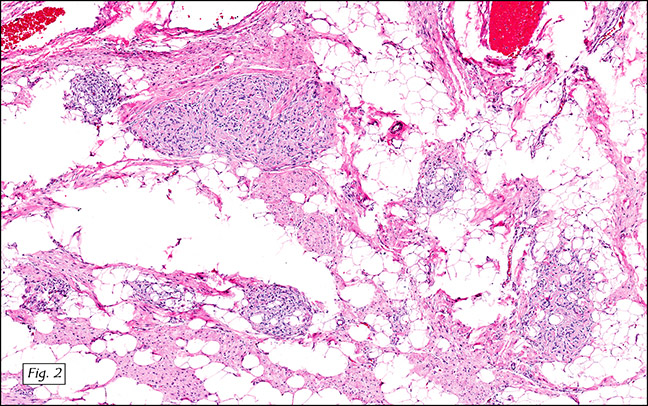
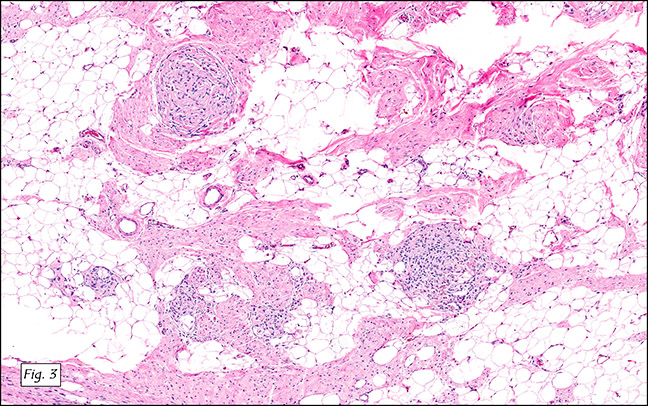
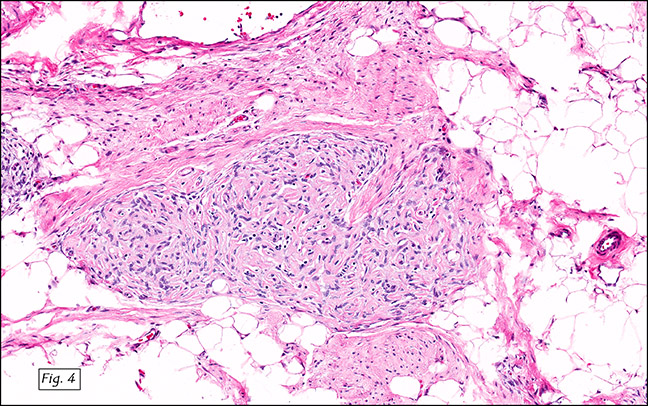
Microscopically the nodule involved the subcutis (Fig. 1) and consisted of an admixture of mature adipose tissue, intersecting trabeculae of fibrous tissue with mature spindle-shaped cells and collagen bundles (Figs. 2, 3). It also showed loosely textured “organoid†areas of myxoid matrix with densely packed round to spindle shaped cells (Figs. 2–4). Neither muscular elements nor cellular atypia were seen.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Fibrous Hamartoma of Infancy
Maral Rahvar, M.D; Donald R Chase, M.D
Department of Pathology and Human Anatomy,
Loma Linda University Medical Center,
Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Fibrous hamartoma of infancy (FHI) is an uncommon benign fibroproliferative tumor of mesenchymal origin. The entity was first described by Dr. Reye in 1956 as “subdermal fibromatous tumor of infancyâ€. The current term, FHI, was proposed in 1965 by Dr. Enzinger who described 30 cases from the files of the Armed Forces Institute of Pathology (AFIP). The newer term is currently preferred because of its emphasis on organoid microscopic appearance, and frequent occurrence in childhood and infancy.
FHI is most common in the first two years of life and often presents as a rapid growing mass in the subcutis or reticular dermis. Although it is usually freely movable, it may be fixed to subcutaneous fascia. Boys are affected two to three more times than girls. It does not spontaneously regress.
The most common location is anterior or posterior shoulder fold, but FHI has also been reported in the upper arm, thigh, shoulder, back and forearm. It mainly presents as a solitary lesion but can be multiple.
Grossly, FHI is poorly circumscribed, firm, grey-white with intermixed irregular small islands of yellow fat. The proportion of adipose to fibrous tissue varies from case to case. In lesions where fat occupies a large portion of tumor, the specimen may resemble a fibrolipoma. The tumor is usually about 4 cm in greatest diameter, but masses as large as 15 cm have been reported.
Histologically, FHI is recognized by the presence of three components forming an organoid pattern:
(1) intersecting trabeculae of fibrous tissue composed of spindle-shaped cells separated by collagen bundles,
(2) loosely textured areas consisting of immature round or stellate cells in a matrix of Alcian blue-positive hyaluronidase sensitive material, and a
(3) varying amount of mature fat.
Although the diagnosis is usually based on H&E examination, immunohistochemical stains may be helpful. Positive stains may include smooth muscle and muscle-specific actin reactivity in the trabecular component, and CD34 is occasionally expressed in the spindle cells.
Local excision is the preferred treatment and recurrences are unusual. Although the etiology of this tumor is still unknown, some cases have shown cytogenetic abnormalities including complex (6;12,8)(q25;q24.3;q13), reciprocal translocation of t(2;3)(q31;q21) and rearrangement of chromosome 1, 2, 5 and 17.
Suggested Reading:
Reye RDK. Considerations of certain subdermal ‘‘fibrous tumors’’ of infancy. J Pathol 1956; 72: 149–154.
Enzinger FM, Fibrous Hamartoma of Infancy. Cancer. 18, 241–8 (1965).
Ritchie EL, Gonzalez-Crussi F, Zaontz MR Fibrous hamartoma of infancy masquerading as a rhabdomyosarcoma of the spermatic cord. J. Urol. 140(4), 800–1 (1988).
Groisman G, Lichtig C Fibrous hamartoma of infancy: an immunohistochemical and ultrastructural study. Hum. Pathol. 22(9), 914–8 (1991).
Dickey GE, Sotelo-Avila C. Fibrous hamartoma of infancy: current review. Paediatr Dev Pathol 1999; 2: 236–243.
Fetsch JF, Miettinen M, Laskin WB, Michal M, Enzinger FM. A clinicopathologic study of 45 pediatric soft tissue tumors with an admixture of adipose tissue and fibroblastic elements, and a proposal for classification as lipofibromatosis. Am. J. Surg. Pathol. 24(11), 1491–500 (2000).
Imaji R, Goto T, Takahashi Y, Akiyama T, Yamadori I A case of recurrent and synchronous fibrous hamartoma of infancy. Pediatr. Surg. Int. 21(2), 119–20 (2005).
Yoon TY, Kim JW Fibrous hamartoma of infancy manifesting as multiple nodules with hypertrichosis. J. Dermatol. 33(6), 427–9 (2006).
Enzinger FM, Weiss SW. Soft Tissue Tumor; 6th edition. Mosby; 2013, 9: 257-283.