History: A 69-year-old man presented with a slowly growing mass in the right knee. Twenty years prior he had trauma to the area and subsequently developed “arthritis†at the site. Physical exam demonstrated the mass but noted that the knee still had full range of motion without pain. MRI showed a 9.8 x 3.8 x 4.4 cm mass with a fat signal at the lateral knee that involved soft tissue and spared the bone. A previous biopsy had been called “lipomaâ€.
The excised specimen weighed 93 grams and was 10.0 x 5.0 x 3.5 cm. It was multi-nodular with a thin capsule. Villous projections of white-yellow adipose tissue were present consisting of white-yellow lobulated adipose tissue. A central portion showed a 2.0 x 1.8 cm region of calcification.
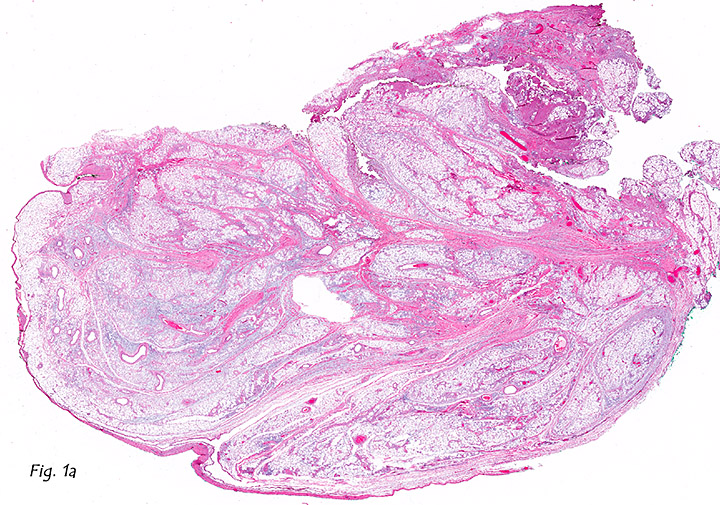
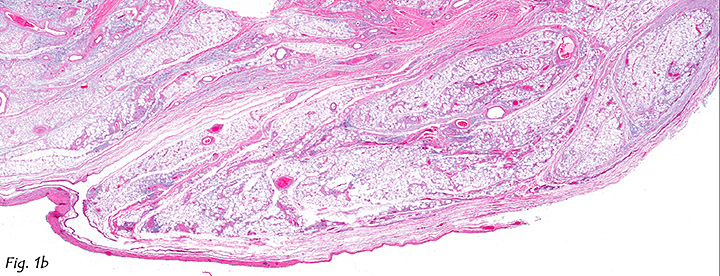
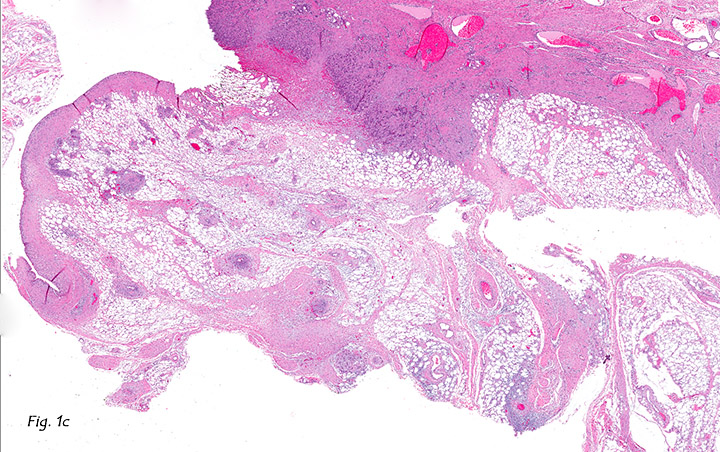
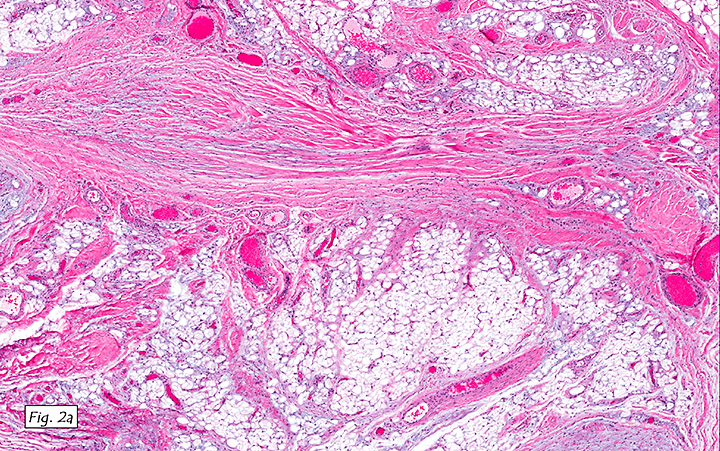
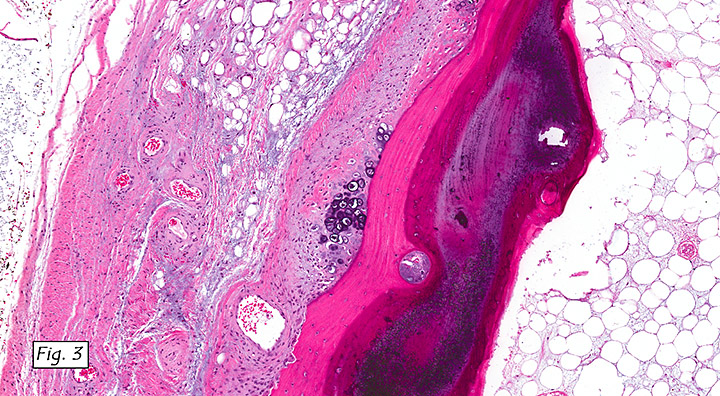
Microscopically, tenosynovial tissues showed well-delimited villous projections of fibrofatty tissue (Figs. 1a, 1b, 1c). Tendon tissue was closely associated with mature fat (Figs. 2a, 2b) There was also a region of osteochondromatous metaplasia (Fig. 3). Neither atypia nor mitotic figures were seen.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis:
Tenosynovial Lipoma Arborescens with Osteochondromatous, Metaplasia, Knee
Tae Hun Kim, MSIV and Donald R. Chase, M.D.
Department of Pathology and Human Anatomy,
Loma Linda University Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Lipoma arborescens (LA) is a rare benign intra-articular lesion characterized by distension of synovial tissue by mature adipose cells. The resulting frond-like appearance was described and coined by Hoffa as “lipoma arborescens†because it reminded him of leaves in a tree.
Lipoma arborescens arises predominantly in adults in their fifth to seventh decade of life with a few occurrences in young adults. It most commonly affects the suprapatellar region of the knee. Other locations have included shoulder, hip, and elbow. The typical presentation is a slowly progressive swelling of the involved joint which may be associated with effusions, pain, and/or decreased range of motion.
Although the etiology remains unclear, associations with chronic joint pathology are usually present. Using MRI, Vilanova et al. found LA to almost always be associated with joint effusion, degenerative changes, meniscal tear, synovial cysts, bone erosions, or synovial chondromatosis. Because of these associations, and noting that complete healing usually occurs after synovectomy, some authors have proposed that LA represents an unusual synovial reactive response to chronic irritation and have suggested a non-neoplastic term “villous lipomatous proliferation of the synovial membraneâ€.
MRI is the image modality of choice and generally shows a frond-like synovial mass with high signal intensity of fat. Grossly, the lesion demonstrates villous projections composed of lobulated yellow adipose tissue. Histologic analysis characteristically shows elongated synovial folds distended by benign adipose tissue without atypia or malignancy. Osseous and/or chondroid metaplasia may also be present.
The differential diagnosis for lipoma arborescens is fairly limited due to its characteristic MRI, gross and microscopic appearances. However, lipoma of tendon sheath should be considered. Lipoma of tendon sheath is a benign tumor of mature adipose tissue attached to a tendon. It is very rare and occurs in young adults in their 5th decade. In contrast to lipoma arborescens, lipoma of tendon sheath is not intraarticular, affecting the tendons of the hands and wrists and, less commonly, the foot and ankle.
Suggested Reading:
Coll JP, Ragsdale BD, Chow B, Daughters TC. Lipoma Arborescens of the Knees in a Patient with Rheumatoid Arthritis. Radiographics. 2011 Mar-Apr;31(2):333-7.
Hallel T, Lew S, Bansal M. Villous lipomatous proliferation of the synovial membrane (lipoma arborescens). J Bone Joint Surg Am. 1988 Feb;70(2):264-70.
Kempson RL, Fletcher CDM, Evans HL, Hendrickson MR, Sibley RK. Atlas of Tumor Pathology: Tumors of the Soft Tissue, 3rd Series Fascicle 30: Washington, D.C., Armed Forces Institute of Pathology, 1998: 191.
Kloen P, Keel SB, Chandler HP, Geiger RH, Zarins B, Rosenberg AE. Lipoma arborescens of the knee. J Bone Joint Surg Br. 1998 Mar;80(2):298-301.
Vilanova JC, Barceló J, Villalón M, Aldomà J, Delgado E, Zapater I. MR imaging of lipoma arborescens and the associated lesions. Skeletal Radiol. 2003 Sep;32(9):504-9.
Weiss S, Goldblum J. Enzinger & Weiss’ Soft Tissue Tumors, 5th ed: Philadelphia, Mosby/Elsevier Inc, 2008; 469-470.