History: A painful, one cm nodule was found the subcutaneous tissue of the right heel of an adult male. Radiographs showed it to be ill-defined and radio-opaque. The nearest bone was the calcaneus, but it was not involved. There was no history of trauma.
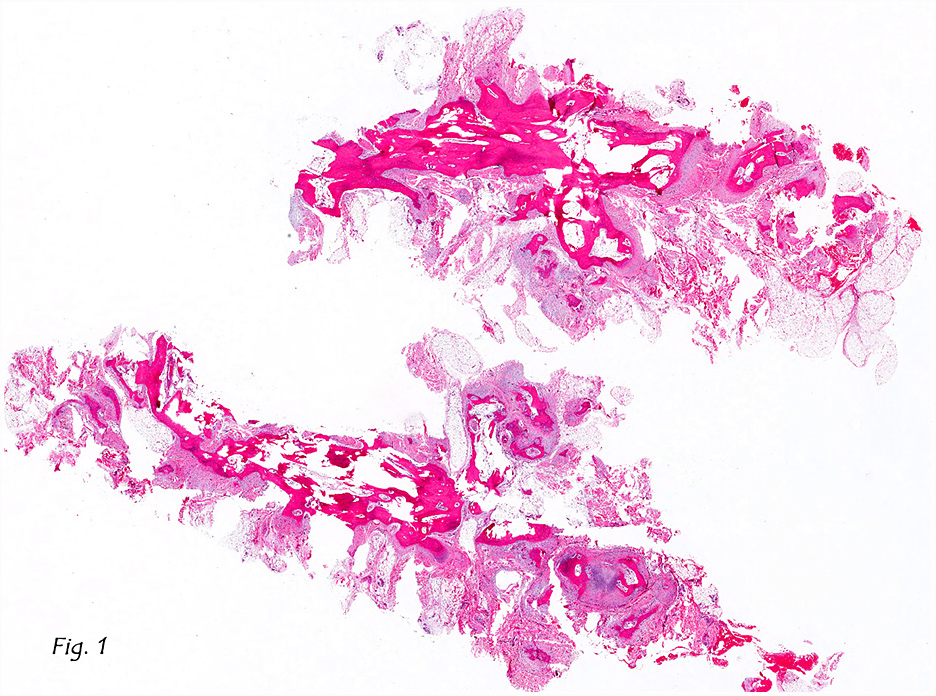
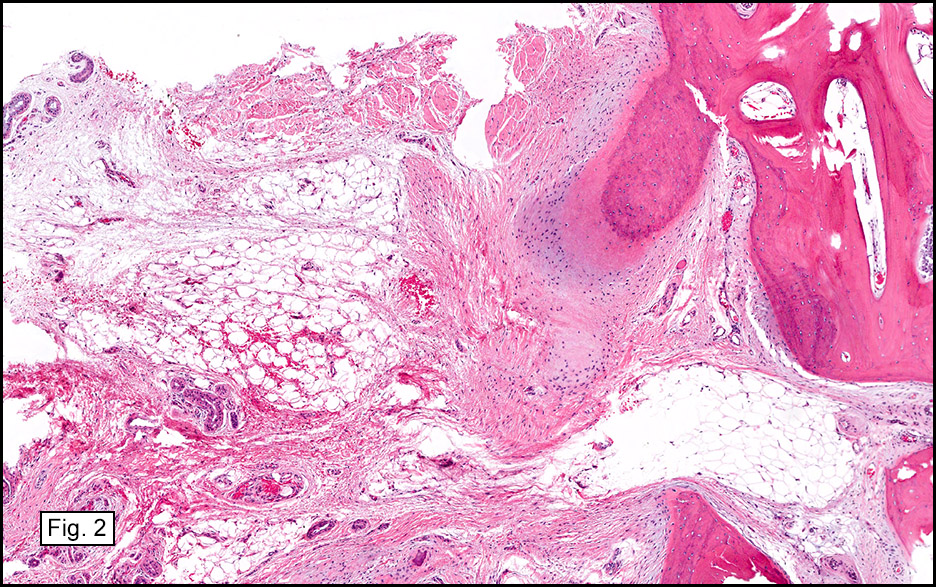
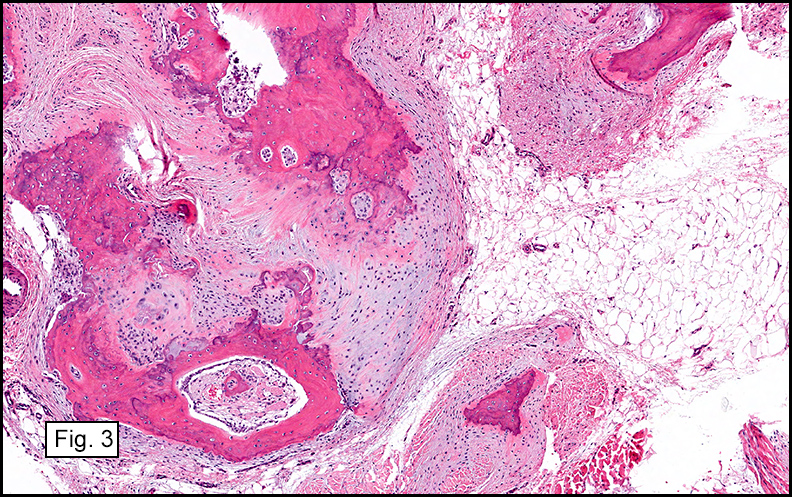
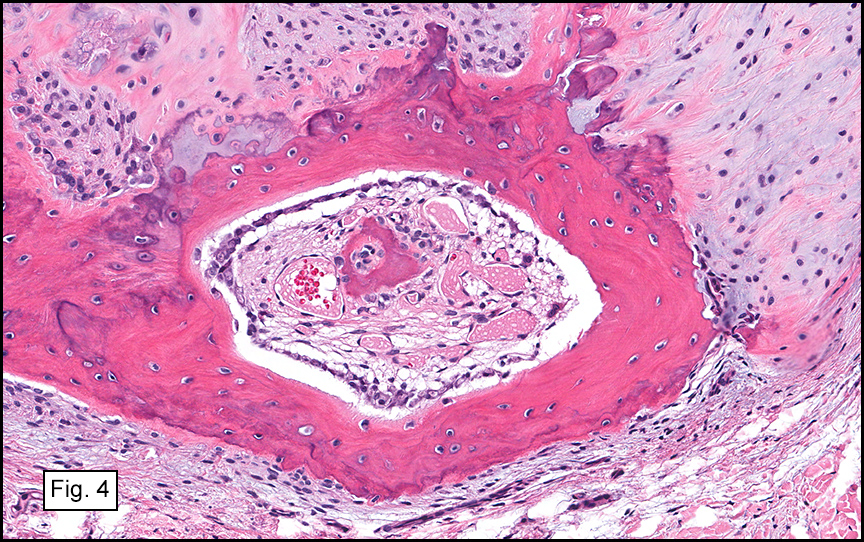
The lesion, at low magnification, consisted of an admixture of adipose tissue, osteoid, trabecular mature bone, and fibrous stroma (Figs. 1, 2). Prominent osteoid, bone and abortive cartilaginous elements were present (Fig. 3). Zones of osteoid were surrounded by cellular or myxoid fibrous stroma and were sometimes rimmed by osteoblasts (Fig. 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Panniculitis Ossificans, heel
Bing Wang, M.D., and Donald R. Chase, M.D.
Department of Pathology and Human Anatomy
Loma Linda University Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
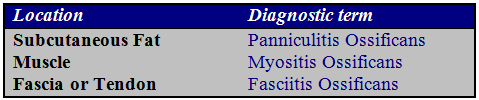
Discussion: Panniculitis Ossificans (PO) is also referred to as a “fibro-osseous lesion†or “heterotopic ossificationâ€. It has been subclassified based upon its location [1]:
Unlike usual panniculitis, which may show inflammatory infiltrates involving the septa [4], PO commonly lacks inflammation. If inflammation is present it is usually minimal and mostly evident in the tissue surrounding the lesion [2].
PO usually affects young, physically active adolescents and adults. Most cases involve the limbs, and some are seemingly incited by injury. The initial symptoms may include pain or tenderness followed by soft tissue swelling. Later, the swollen tissue becomes circumscribed and indurated. Calcification usually starts three to six weeks following injury [2].
Radiographs show a series of changes, initially with an increase in soft tissue density or opacity. Calcification starts around the end of third week, and as the lesion becomes increasingly calcified, it becomes well-circumscribed with either a solitary region of calcification or scattered regions of calcification [2].
Histologically, PO is usually well-circumscribed and is characterized by the presence of a distinct zonal pattern that reflects different components of this entity, including: normal-appearing adipose tissue, fibrous stroma, osteoid and mature bone. The adipose tissue consists of normal lobules of mature fat. Fat necrosis usually is not seen. Foci of osteoid formation are scattered between the lobules of adipose tissue, and are usually surrounded by a cellular or myxoid fibrous stroma. Trabeculae of mature bone usually begins in the middle of osteoid islands. The content of the mature bone formation depends on the stage of the lesion. Sometimes osteoid and mature bones are rimmed by layers of osteoblasts showing little variation in size and shape. The osteoid and bone are separated from the surrounding tissue by a zone of loose or compressed fibrous tissue. The fibrous tissue consists of fibroblasts and myofibroblasts which may display a mild degree of cellular pleomorphism and rather prominent mitotic activity. In addition, there may be prominent vascular proliferation, focal hemorrhage, or fibrin deposition [2].
Panniculitis ossificans is a benign lesion and its etiology is not fully understood. It is usually caused by some kind of injury. It is proposed that injuries may generate an environment which produces certain proteins such as bone morphogenic protein, which in turn, can induce pluripotential mesenchymal cells to turn into osteogenic cells, which can then form osteoid, which in turn develops into mature heterotopic ossification [3].
There is no convincing evidence of malignant transformation of panniculitis ossificans [2]. The early stage of PO has immature and highly cellular zones that may be confused with extraskeletal osteosarcoma. However, extraskeletal osteosarcoma usually occurs in older patients; in contrast panniculitis ossificans often occurs in younger active people. Unlike panniculitis ossificans, extraskeletal osteosarcoma shows marked cellular atypia and infiltration of neighboring tissues in a destructive manner. Panniculitis ossificans is well-circumscribed with distinct zones of different components. In some cases, PO may contain entrapped atrophic muscle, which may cause confusion with another entity in the same category, myositis ossificans. The difference lies in how much muscle or adipose tissue is present in the lesion [2].
Suggested Reading:
1. Ackerman LV. Extra-osseous localized non-neoplastic bone and cartilage formation (so – called myositis Ossificans): clinical and pathological confusion with malignant neoplasms. J Bone Joint Surg Am 1958; 40-A(2): 279-298.
2. Goldblum JR, Folpe AL and Weiss SW. Soft tissue tumors, sixth edition. Pg 926-932.
3. McCarthy EF, Sundaram M: Heterotopic ossification: a review. Skeletal Radiol.34:609-619 2005.
4. Requena L. Normal subcutaneous fat, necrosis of adipocytes and classification of the panniculitides. Semin Cutan Med Surg 2007; 26:66–70.