History: A 70-year-old male presented with a one year history of nasal obstruction, facial pain, occasional epistaxis, and headache. A CT scan of the head found a 5.0 x 3.0 cm heterogeneous mass in the left frontal lobe. A biopsy was performed.
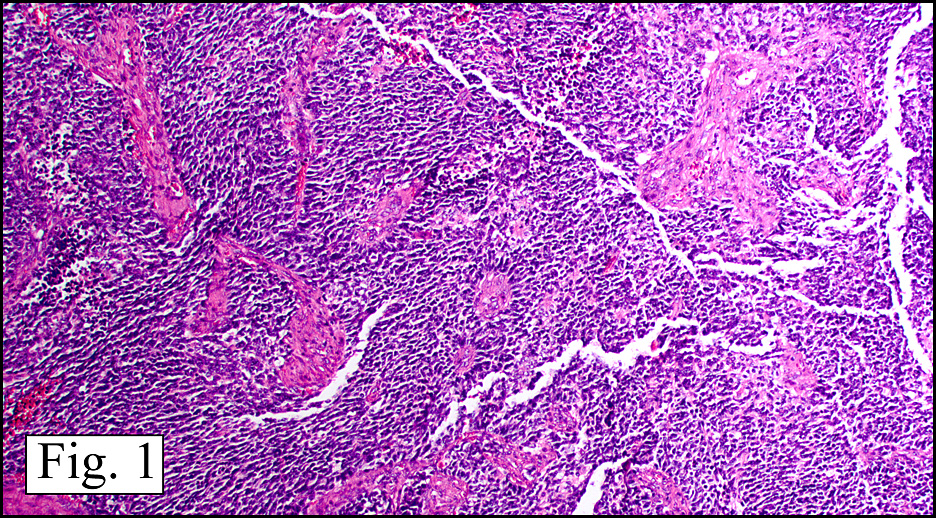
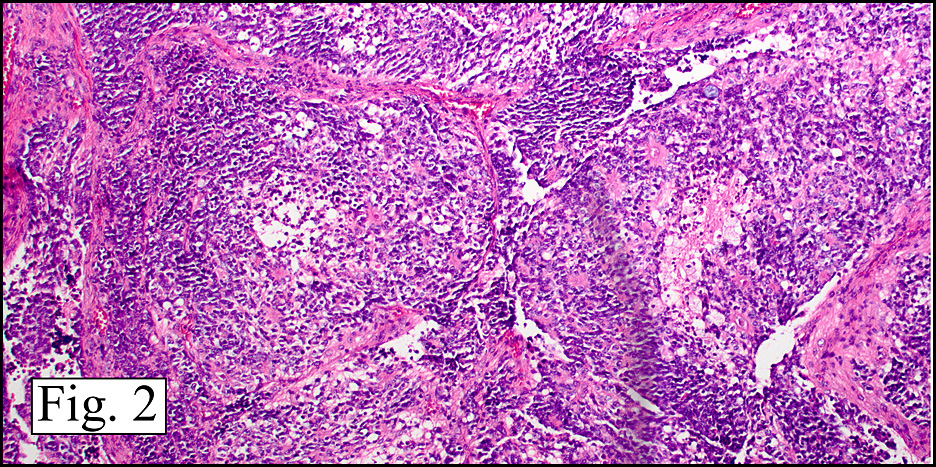
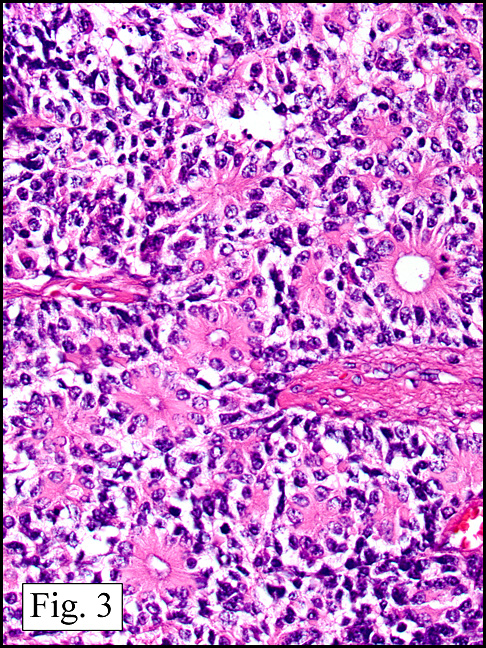
Microscopically, the lesion consisted of irregular nests and sheets with fibrovascular stroma (Fig. 1) consisting of uniform small cells containing scant cytoplasm and round to ovoid nuclei with indistinct nuclear membranes, punctuate chromatin and indistinct nucleoli. A fibrillary or reticular background was seen in some areas with others demonstrating more diffuse sheets of cells with a little intervening stroma (Fig. 2). Rosettes of variable size with delicate neurofibrillary stroma and palisading tumor cells were identified with and without lumens (Fig. 3). Immunohistochemically, the tumor cells were positive for S100 and NSE and negative for chromogranin. The rosettes stained positively for keratin but were GFAP negative, while occasional tumor cells and adjacent glial cells were positive for GFAP.
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Olfactory Neuroblastomaâ€
Jin Guo, MD, Amita Mistry MD and Donald R. Chase, MD
Department of Pathology, Loma Linda University and Medical Center,
Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Olfactory neuroblastoma (esthesioneuroblastoma) is a rare malignant tumor of neuroectodermal origin accounting for 1 to 5% of malignant neoplasms in the nasal cavity. Occurring in all age groups (3-88 years) with bimodal peaks in the second and fifth decades, there is no gender predilection. Fewer than 1,000 cases have been reported in the literature since the tumor was first described more than 75 years ago. The tumor is thought to arise from the specialized sensory neuroepithelial (neuroectodermal) olfactory cells in the superior one third of the nasal cavity, including the cribriform plate of the ethmoid sinus as well as the superior turbinate. Almost all olfactory neuroblastomas involve the cribriform plate to some degree, and even when the bulk of a tumor lies intracranially, as in the current case, it is often still attached to the cribriform plate. Patients often present with nonspecific symptoms such as unilateral nasal congestion or obstruction (70%), recurrent epistaxis (50%) and, less commonly, facial pain, headache, anosmia, visual disturbances and/or diplopia. Because of the nonspecific nature of the presenting symptoms, the diagnosis is often missed during its early stages and may not be made until an advanced stage.
Morphologically, olfactory neuroblastoma is characterized by lobular architecture with circumscribed islands or nests of primitive neuroblastoma cells in a vascularized fibrous and fibrillary stroma. The tumor cells are small and round with a blue appearance and a high nucleus-to-cytoplasm ratio. Small and uniform nuclei have an even distribution of granular chromatin and often contain inconspicuous nucleoli. Nuclear pleomorphism, increased mitotic figures and necrosis are uncommon, but may be present in the high grade tumors. Tumor cells are often arranged in a syncytial pattern forming epithelial tubules or rosettes which sometimes resemble that of an ependymoblastoma. Immunohistochemically, the tumor cells stain positive for neuron-specific enolase, synaptophysin, chromogranin, neurofilament, catecholamines and S100 (sustentacular distribution), while staining negatively for EWS-FL1, CD99, EMA and desmin. Since chromogranin can be negative, alone it neither proves nor disproves the diagnosis of neuroblastoma. GFAP positivity is often restricted through active gliosis and occasional GFAP positivity in the tumor cells may indicate the presence of some degree of glial differentiation. The diagnosis of olfactory neuroblastoma is often established through histopathology accompanied by clinical and demographic findings, and then confirmed with pertinent immunohistochemical studies.
The degree of differentiation combined with the presence or absence of a neural stroma, mitotic figures and necrosis determines the grade (I through IV) of an olfactory neuroblastoma. Higher-grade tumors are poorly differentiated and characterized by more pleomorphic nuclei with coarser chromatin, increased mitoses, and necrosis. Pseudorosettes and fibrillar stroma are less commonly seen. Histological grade correlates with the prognosis, although not as closely as tumor stage. Stage A tumors are limited to the nasal cavity, stage B tumors involve the nasal cavity and paranasal sinuses, and stage C tumors extend beyond these structures. At presentation, approximately one-half of all olfactory neuroblastomas are stage C tumors.
Owing to the “small, round, blue-cell” morphology of this neoplasm, the differential diagnosis is quite extensive:
- Neuroendocrine carcinomas of the nasal cavity and nasal sinuses are especially uncommon and thought to originate from the glandular epithelium of the exocrine glands found in normal olfactory mucosa. Often occurring in older patients (mean age 50 years), these tumors seldom involve the cribriform plate and are composed of sheets and nests of small to intermediate-sized cells with a high nuclear-cytoplasmic ratio, hyperchromatic nuclei, and high mitotic rates.
- Sinonasal undifferentiated carcinomas were first recognized as a distinct entity in 1986, and are comprised of medium-sized cells arranged in nests and sheets with wide trabeculae, extensive necrosis and vascular permeation. Prognosis is considerably less favorable than for olfactory neuroblastoma.
- Pituitary tumors involving the paranasal sinuses frequently arise secondary to invasion from an intrasellar tumor rather than from an ectopic focus. These neoplasms share the wide histological spectrum of other pituitary adenomas, ranging from lesions with neuroendocrine features to those resembling poorly differentiated carcinomas. Sinonasal pituitary adenomas in general may be more aggressive than regular pituitary adenomas because they are commonly more invasive macroadenomas.
- Lymphomas arising from the paranasal sinuses are distinctly less common in Western than in Asian populations, accounting for less than 1% of all extranodal malignant lymphomas. Virtually every subtype of lymphoma can occur in the paranasal sinuses with B-cell lymphomas and natural killer/T-cell lymphomas more regularly encountered. There is an increased male to female ratio with most cases occurring in the sixth to eighth decades of life.
- Sinonasal melanoma, which migrates from the neuroectoderm, is an uncommon tumor constituting 4.8% of all neoplasms in this region. It is composed of a variable morphology of cells that may be round, oval, polygonal, epithelioid, or spindle shaped. Predominantly developing in patients in their fifth through eighth decades of life, these tumors are aggressive with a 5-year survival rate of 36%.
- Despite that facial rhabdomyosarcoma is relatively uncommon, it should be considered in the presence of a rapidly growing facial swelling which is unresponsive to antibiotics. Histologically, the tumor consists of solid sheets of small cells with scattered foci lining alveola-like spaces. Immunohistochemical studies demonstrate the presence of desmin and myoglobin, and absence of pre-keratin, neuron-specific enolase, and leukocyte common antigen (LCA).
- Ewing sarcoma and primitive neuroectodermal tumors (PNET) have a characteristic profile with diastase sensitive PAS positivity, and positive staining for CD99, FLI1 protein NSE, and CD57. Negative staining is seen for S100, LCA, muscle and vascular markers. These tumors routinely share the cytogenetic translocation t (11;22) (q24;q12). Though morphologically similar, it is controversial whether olfactory neuroblastoma and Ewing’s sarcoma/PNET carry the same cytogenetic translocations.
- Plasmacytomas and paragangliomas should also be considered as part of the differential investigation. The distinction of high-grade olfactory neuroblastoma from other poorly-differentiated neoplasms arising in the nasal cavity is challenging and essential to determining patient management and prognosis. A future potential diagnostic marker could be based upon the human achaete-scute homologue (hASH1) gene which is critical in olfactory neuronal differentiation and expressed in immature olfactory cells.
Even though diagnostic and treatment modalities have improved over the past two decades, limited data exists with respect to optimum management strategies due to the rare nature of olfactory neuroblastomas. The natural history of the disease, which may range from slow progression to aggressive local recurrence and distant metastasis, has yielded various treatment protocols and recommendations. Current consensus recommendation for treatment of primary low to moderate-grade tumors is radical craniofacial resection followed by radiotherapy with the addition of chemotherapy for patients with advanced, recurrent, or metastatic disease. Approximately 15% of patients acquire cervical lymph node metastasis, and 10% develop a distant metastasis at some point during the course of their disease. The 5-year survival rate varies from 45 to 80% based on different studies with a local recurrence rate of 30%. Overall negative prognostic factors include age (greater than 50 years at presentation), advanced stage or grade, tumor recurrence, and metastasis.
Suggested reading:
Porter AB, Bernold DM, Giannini C, Foote RL, Link MJ, Olsen KD, Moynihan TJ, Buckner JC. Retrospective review of adjuvant chemotherapy for esthesioneuroblastoma. J Neurooncol. 90(2):201-4. 2008.
Bumm K, Grizzi F, Franceschini B, Koch M, Iro H, Wurm J, Ceva-Grimaldi G, Dimmler A, Cobos E, Dioguardi N, Sinha UK, Kast WM, Chiriva-Internati M. Sperm protein 17 expression defines 2 subsets of primary esthesioneuroblastoma. Hum Pathol. 36(12):1289-93, 2005.
Zvi R. Cohen, M.D., Eric Marmor, M.D., Gregory N. Fuller, M.D., Ph.D., and Franco Demonte, M.D. Misdiagnosis of Olfactory Neuroblastoma. Neurosurg Focus. 2(5). 2002.
Dulguerov P, Allal AS, Calcaterra TC. Esthesioneuroblastoma: A metaanalysis and review. Lancet Oncol. 2:683-90. 2001.
Miyamoto RC, Gleich LL, Biddinger PW, Gluckman JL. Esthesioneuroblastoma and sinonasal undifferentiated carcinoma: impact of histological grading and clinical staging on survival and prognosis. Laryngoscope. 110:1262-1265. 2000.
Eriksen JG, Bastholt L, Krogdahl AS, et al. Esthesioneuroblastoma — what is the optimal treatment? Acta Oncol. 39:231-235. 2000.
Mezzelani A, Tornielli S, Minoletti F, Pierotti MA, Sozzi G, Pilotti S. Esthesioneuroblastoma is not a member of the primitive peripheral neuroectodermal tumour-Ewing’s group. Br J Cancer. 81:586-591. 1999.
Broich G, Pagliari A, Ottaviani F. Esthesioneuroblastoma: a general review of the cases published since the discovery of the tumour in 1924. Anticancer Re. 17:2683-2706. 1997.
Hirose T; Scheithauer BW; Lopes MB; Gerber HA; Altermatt HJ; Harner SG; VandenBerg SR. Olfactory neuroblastoma. An immunohistochemical, ultrastructural, and flow cytometric study. Cancer. 1;76(1):4-19. 1995.
Whang-Penn J. Translocation t (11:22) in esthesioneuroblastoma. Cancer Genet Cytogenet. 1:155-159. 1987.
Thompson L. Olfactory neuroblastoma. Ear Nose Throat J. 85(9):569-70. 2006.