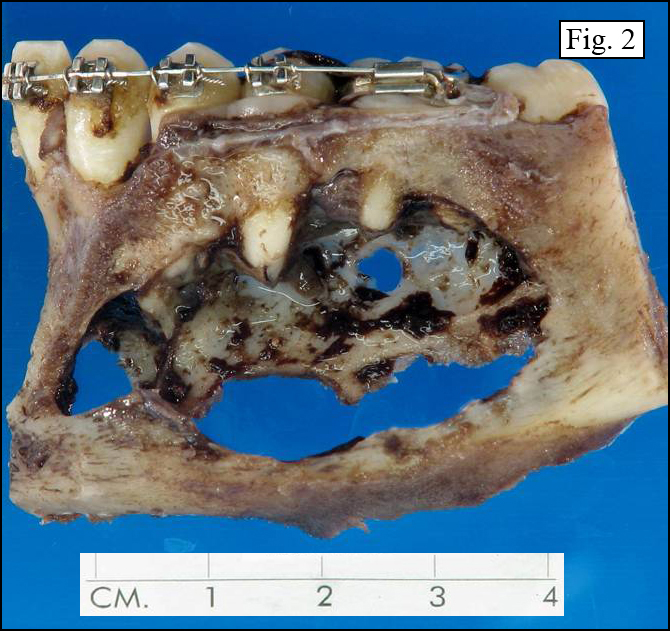
History: A 16 year-old boy presented to his orthodontist with a two-year history of left mandibular swelling. An x-ray showed a well-circumbscribed radiolucent lesion of the left body of mandible extending from teeth #18-22 (Fig. 1). The left mandibulectomy specimen contained a 4.2 x 2.2 cm cystic lesion (Fig. 2). Tissue removed from the cyst consisted of loosely adherent pink-brown soft-tissue fragments with focal areas of necrosis.
{kind=link}
{kind=link}
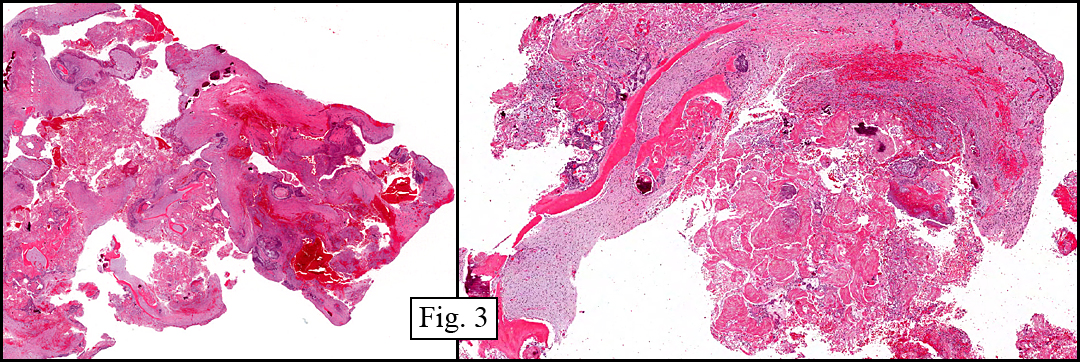
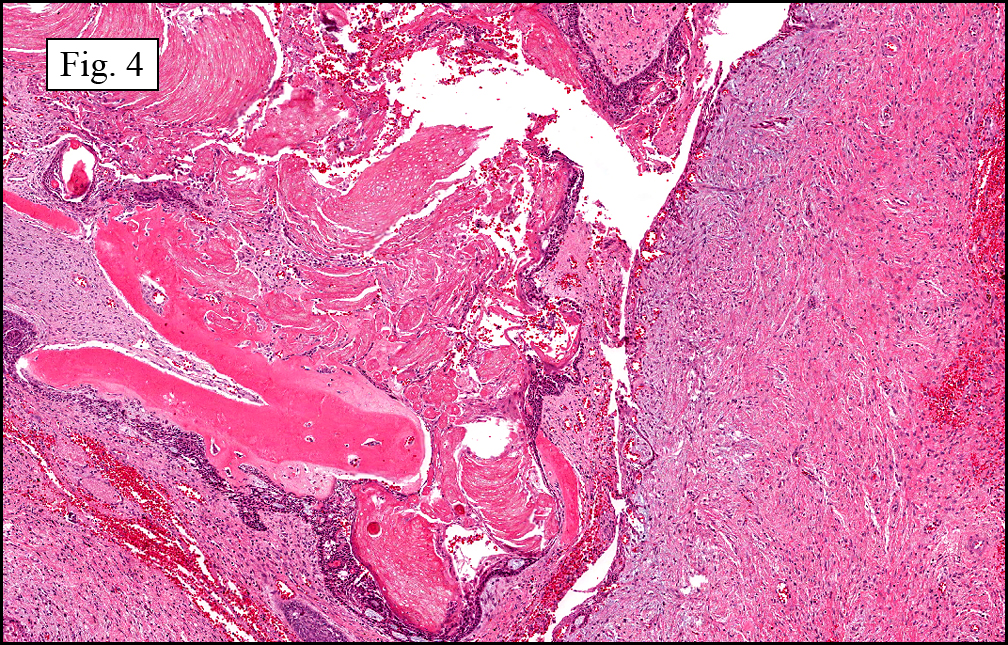
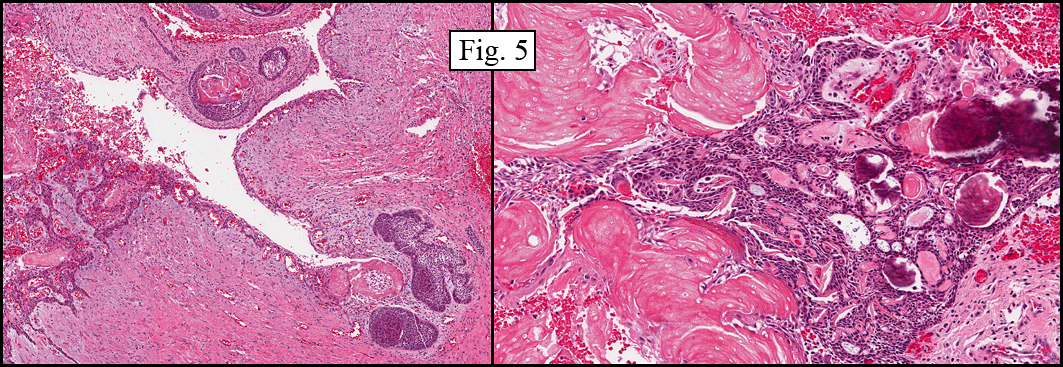
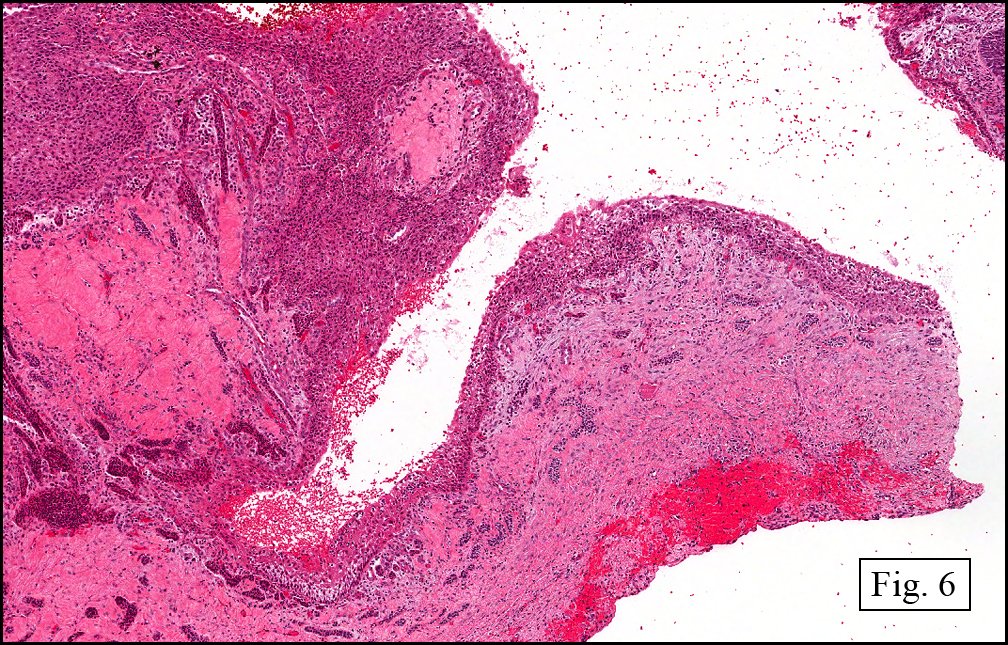
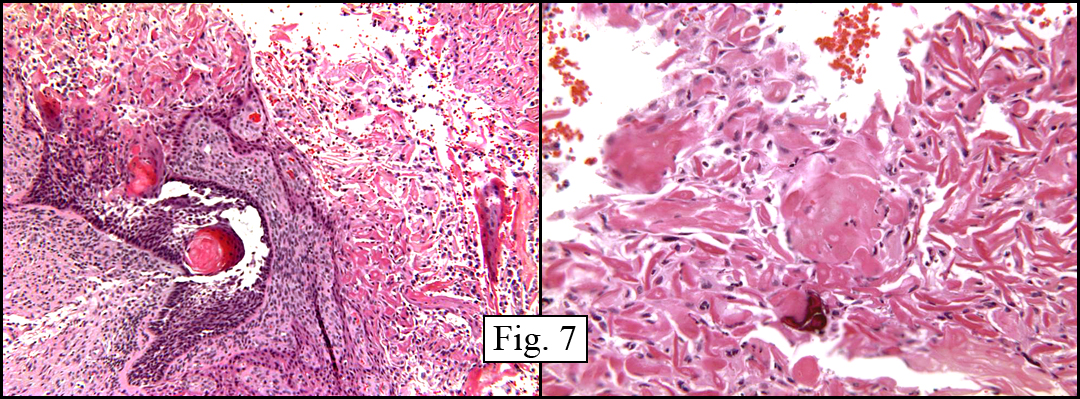
The tumor consisted of an admixture of trabecular bone and hemorrhagic fibrous tissue (Fig. 3). A cystic lining was composed of squamoid elements with a prominent basal component (Fig. 4, 5, 6). Aggregates of “ghosted epithelium†were present throughout (Fig. 4, 5, 7) as were areas of ameloblastic-type epithelium (Fig. 5). Focally calcified keratinaceous debris was seen, sometimes associated with basaloid epithelium (Fig. 7). Adjacent soft tissues showed regions of tooth germinal epithelium with tooth-like pulp stroma, with occasional amounts of eosinophilic material consistent with dentin.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Calcifying Odontogenic Cyst (‘Keratinizing and Calcifying Odontogenic Cyst’, ‘Gorlin Cyst’) with associated early odontoma formationâ€
Justin Kerstetter, MD, Craig Zuppan, MD, and Donald R. Chase, MD
Department of Pathology and Human Anatomy, Loma Linda University and Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Calcifying odontogenic cyst (COC), classified as an odontogenic tumor by the World Health Organization (WHO), was first identified as a distinct entity by Gorlin et al. in 1962, and now is felt to be a true neoplasm. These lesions arise from a more mature enamel epithelium than ameloblastoma and accordingly appear to have less growth potential. After Gorlin’s first description, COC was re-labeled as a “calcifying ghost cell odontogenic tumor†by Fejerskov and Krogh in 1972, and now is sometimes referred to as a “Keratinizing and Calcifying Odontogenic Cystâ€. The tumor usually arises in younger adults with most cases diagnosed in the second to third decades, but patients may range in age from infant to adult. COC is predominantly an intraosseous tumor although approximately 13-30% of the cases occur as extraosseous lesions. Both intraosseous and extraosseous lesions occur with equal frequency in the maxilla and mandible with about 65% of the cases being found in the incisor and canine areas.
In addition to the histologic features described in this case, calcifying odontogenic cysts are well-defined with a fibrous capsule and a lining of odontogenic epithelium of 4 to 10 cells in thickness. The basal cells may be cuboidal or columnar and resemble ameloblasts. The most characteristic feature of this tumor is variable numbers of ghost cells within the epithelial component. These cells are altered epithelial cells showing loss of their nuclei with preservation of basic cell outline. Finally, COC may be associated with other odontogenic tumors, with odontoma being the most common. However, other tumors reported in association with COC include ameloblastomas and adenomatoid odontogenic tumors.
The differential diagnosis of COC includes:
• Dentigerous cysts may be associated with unerupted teeth. They originate from the separation of the follicle from around the crown of the unerupted tooth and remain attached to the tooth which remains in the alveolar bone. Histologically, they demonstrate a fibrous capsule with a thin, non-keratinized epithelial lining. These cysts may demonstrate an inflamed or non-inflamed appearance based on the presence of a chronic inflammatory cell infiltrate.
• Eruption cysts are the soft-tissue variant of the dentigerous cyst. Their origin is also from the separation of the dental follicle from the crown of an erupting tooth that is within the soft tissue overlying the alveolar bone. Histologically there is the presence of oral epithelium overlying the roof of the cyst which is comprised of a thin layer of nonkeratinizing squamous epithelium.
• Odontogenic keratocysts arise from cell rests of the dental lamina and are associated with Gorlin syndrome when they are multiple. The luminal surface of the cyst demonstrates flattened, parakeratotic epithelium which is wavy or corrugated in appearance. The basal epithelial layer is composed of a palisaded layer of cuboidal or columnar epithelial cells which are hyperchromatic. These have a tendency to recur.
• Glandular odontogenic cysts occur mainly in the anterior portion of the mandible. They are lined by squamous epithelium of varying thickness. The superficial epithelial cells lining the cyst cavity are cuboidal to columnar and have an irregular, sometimes papillary surface. Pools of mucinous material are often present within the epithelium.
Suggested Reading:
Calcifying odontogenic cyst – a possible analogue of the cutaneous calcifying epithelioma of Malherbe (an analysis of fifteen cases). Gorlin RJ, Pindborg JJ, Clausen FlP et al. Oral Surg, 15:1235-1240, 1962.
Syndromes of the Head & Neck, by Gorlin RJ and Pindborg, McGraw-Hill, New York, 1964.
The calcifying ghost cell odontogenic – or the calcifying odontogenic cyst. Fejerskov O, Krogh J. J Oral Pathol, :273-287, 1972.
Calcifying odontogenic cyst associated with odontoma: report of two cases. Keszler A, Gugliemontti NB. J Oral Surg, 30:893-897, 1972.
Calcifying odontogenic cyst. A review and analysis of seventy cases. Freedman PD, Lumerman H, Gee JK. Oral Surg, 40:93-106, 1975.
The keratinizing and calcifying odontogenic cyst (Gorlin cyst). Clark MJ, Alley RS, Steed DL, Tilson HB. J Am Dent Assoc. 100(4):563-564, 1980.
Calcifying odontogenic cyst: case report and review of literature. el-Beialy RR, el-Mofty S, Refai H. J. Oral Maxillofac Surg, 48(6)637-40, 1990.