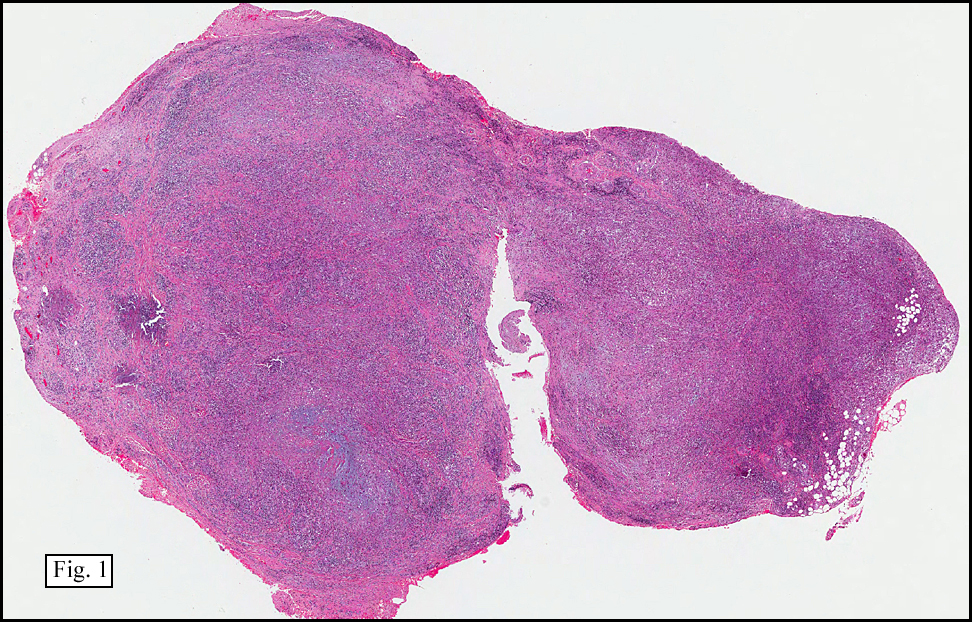
History: A 33 year-old woman presented with a progressively enlarging, tender nodule in the palmar aspect of the right fourth finger. An approximately 1.0 cm diameter, circumscribed, nodular soft tissue mass was removed (Fig. 1).
{kind=link}
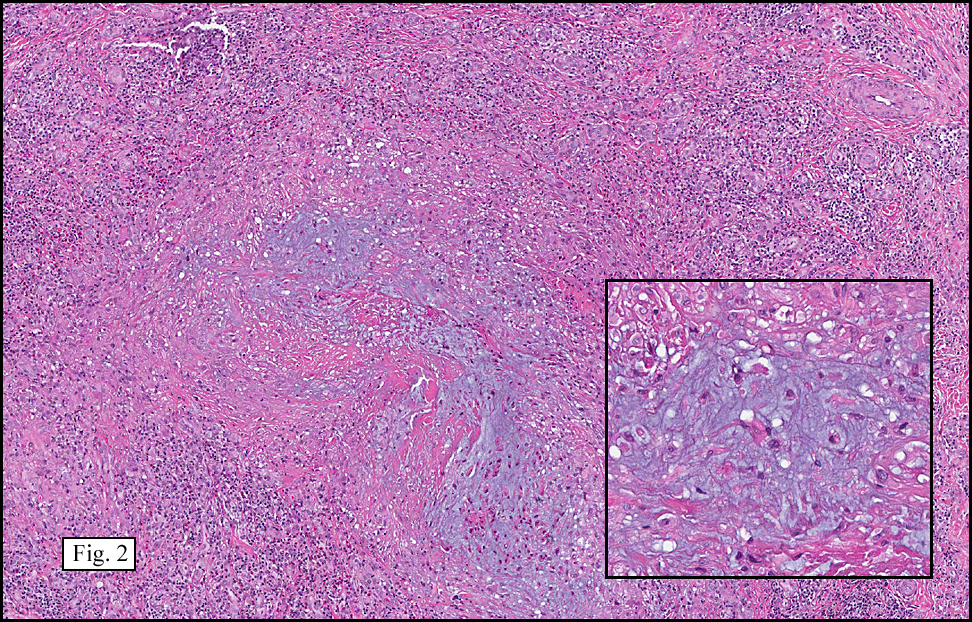
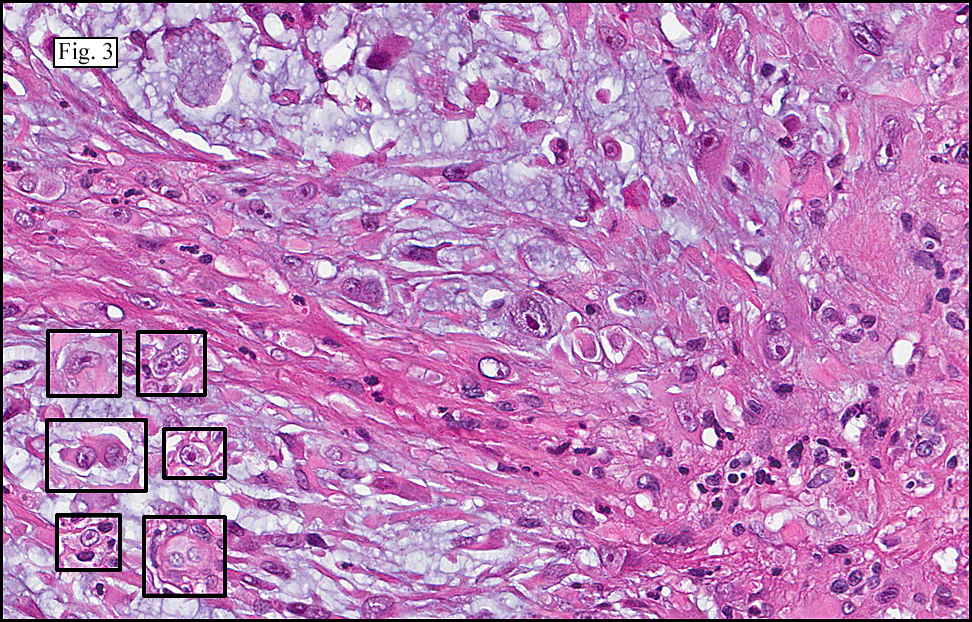
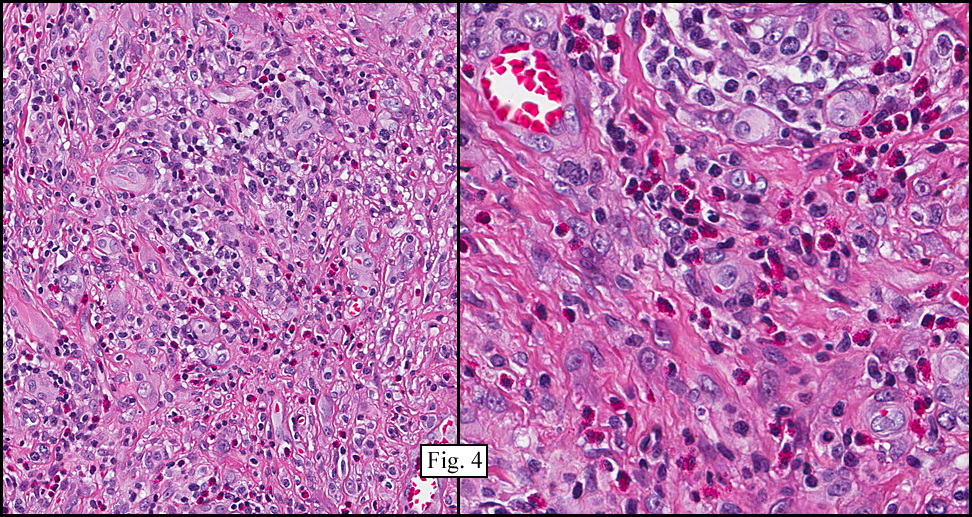
Microscopically, the tumor was composed of spindled and epithelioid cells with oval to rounded nuclei and conspicuous nucleoli prominently supported by alternating undulations of myxoid and hyalinized matrix (Fig. 2). Several of the larger epithelioid cells had abundant eosinophilic cytoplasm, multilobulated nuclei and striking macro nucleoli reminiscent of Reed-Sternberg cells (Fig. 3). In addition, admixed within the mass was a dense chronic inflammatory infiltrate consisting mostly of lymphocytes and plasma cells with occasional areas of numerous eosinophils (Fig. 4). An infrequent multinucleated giant cell was also seen with intermingling round mononuclear cells with bland nuclei and amphophilic cytoplasm.
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical staining revealed limited focal positivity for CD34 and rare positivity for epithelial membrane antigen in the lesional cells. Other cytokeratin markers as well as CD31, or S-100 were negative.
Diagnosis: “Acral Myxoinflammatory Fibroblastic Sarcomaâ€
Brian Willis PSF and Donald Chase MD
Department of Pathology & California Tumor Tissue Registry
Loma Linda University and Medical Center, Loma Linda, California
Discussion: Acral myxoinflammatory fibroblastic sarcoma (AMIFS) is a rare, recently-described soft tissue tumor with just over one-hundred cases reported in the literature. First described in 49 patients by Montgomery and colleagues in 1998, it was originally entitled “Inflammatory myxohyaline tumor of the distal extremities with virocyte or Reed-Sternberg-like cells. The identical tumor was shortly later described by Meiss-Kindblom and Kindblom as “acral myxoinflammatory fibroblastic sarcomaâ€. Included in their presentation cases was a patient with biopsy-proven inguinal lymph node metastasis. The authors added the term “sarcoma†to emphasize the possibility of an aggressive clinical course, and AMIFS became the preferred term.
As reported, AMIFS occurs mostly in adulthood, generally within the fourth and fifth decades, but the age range is likely broader. Males and females are equally affected. The tumor presents as a slowly growing, multinodular, ill-defined mass usually in the fingers and/or hand. Magnetic resonance imaging shows a poorly circumscribed mass with involvement of the underlying tendon sheath; a finding that, when coupled with the location, leads to the preliminary diagnostic consideration of ganglion cyst or tenosynovitis.
Microscopically, there is usually a dense inflammatory infiltrate mostly composed of an admixture of lymphocytes and neutrophils, plasma cells, and eosinophils insinuated into a background of alternating undulations of myxoid and hyaline stroma. The more cellular zones may have bizarre cells that are spindled, epithelioid, or polygonal. The larger epithelioid cells frequently display prominent, sometimes multilobulated, vesicular nuclei with conspicuous macronucleoli and an abundant eosinophilic cytoplasm, strikingly reminiscent of Reed-Sternberg cells or virocytes. Despite the cytomorphology of these cells, they are negative for CD15/30, and are PCR negative for CMV and EBV. Occasional, ganglion-like cells, multinucleated giant cells, and lipoblast-like cells may also be found within the tumor. Mitotic figures are scarce, despite the relatively high cellularity and high degree of nuclear atypia.
Immunohistochemical findings are essentially non-contributory, with the larger bizarre cells showing consistent immunoreactivity for vimentin and focal, variable reactivity for CD68, CD34, and smooth muscle actin. There may be limited focal immunoreactivity for cytokeratins. S-100, HMB-45, desmin, CD15, and CD30 are virtually always negative. In one recent study by Kovarik and colleagues, diffuse, strong reactivity for CD163 and EGFR was demonstrated. KI-67 positivity is minimal, helping to confirm the low mitotic rate seen on H&E.
Ultrastructurally, the neoplastic cells have abundant endoplasmic reticulum and mitochondria along with large perinuclear whorled deposits of intermediate filaments without actin-type filaments, findings most consistent with a tumor of fibroblastic differentiation.
In the described cases of AMIFS, rates of local recurrence after surgical resection range from 20% to 70%, with approximately one-third of cases eventually necessitating digital amputation. Despite having a low metastatic rate (<2%), distant spread to lymph nodes and lung have been reported. The differential diagnosis of AMIFS includes infectious processes, lymphomas, and other tumors with myxoid or inflammatory characteristics, as well as tumors that arise in the distal extremities, such as giant cell tumor of tendon sheath. • Myxofibrosarcoma/myxoid malignant fibrous histiocytoma represents perhaps the most important distinction in the differential diagnosis. This much higher grade sarcoma shows pleomorphic cells of a degree not seen in AMIFS. Additionally, the myxoid stroma is more uniformly distributed than is seen in AMIFS, and there are not the unusual atypical cells which mimic Reed-Sternberg cells or virocytes. Also, the acral location argues strongly against the diagnosis of myxofibrosarcoma. • Giant cell tumor of the tendon sheath is the most common soft tissue tumor of the fingers. It usually shows numerous Touton-like giant cells along with a lympho-histiocytic cellular infiltrate; however it lacks the large, bizarre, epithelioid cells that characterize AMIFS. • Inflammatory myofibroblastic tumor may be considered based on the presence of a strong inflammatory component in conjunction with a spindle cell background. The presence of the ultrastructural features of myofibroblasts and the lack of bizarre cells precludes this diagnosis in cases of AMIFS. In addition, inflammatory myofibroblastic tumor is seldom encountered in acral locations. • Ganglion cysts and juxta-articular myxomas lack the bizarre, atypical cells of AMIFS. • The presence of Reed-Sternberg-like cells raises the question of Hodgkin’s disease; however, AMIFS does not show positivity for CD15/30. The origin of AMIFS is unknown. Only a few cytogenetic studies have been performed. They have demonstrated a t(1;10) switch with losses of chromosomes 3 and 13 as well as other complex non-specific chromosomal aberrations mostly involving shared gains at chromosome 7. Acral myxoinflammatory fibroblastic sarcoma is a unique slow-growing low-grade sarcoma that presents peculiarly in the distal extremities. Because the complex histology of this lesion may mimic benign inflammatory, reactive changes or even lymphoma careful evaluation is necessary to arrive at the correct diagnosis. Differences in reports of recurrence and metastases likely vary as a result of differences in initial diagnosis, underscoring the importance of proper diagnosis and primary surgical treatment by complete extirpation with clear margins to lower the likelihood of local recurrence or metastases. Suggested Reading
Kovarik CL, Barrett T, et al. Acral myxoinflammatory fibroblastic sarcoma: case series and immunohistochemical analysis. J Cutan Pathol; 2008; 35: 192-196.
Hassanein AM, Atkinson SP, Al-Quran SZ, et al. Acral myxoinflammatory fibroblastic sarcomas: are they all low-grade neoplasms? J Cutan Pathol 2008: 35:186-191.
Baumhoer D, Glatz K, Schulten HG, et al. Myxoinflammatory fibroblastic sarcoma: investigations by comparative genomic hybridization of two cases of and review of literature. Virchow Arch 2007; 451: 923-928.
Gonzalez- Campora R, Rios-Martin JJ, et al. Fine needle aspiration cytology of an acral myxoinflammatory fibroblastic sarcoma: case report with cytological and cytogenetic findings. Cytopathol 2008; 19: 118-123.
Alkuwari E, Gravel DH. A 30-year-old man with a soft tissue mass on the right elbow. Inflammatory myxohyaline tumor of the distal extremeties with prominent eosinophilic infiltrate. Arch Pathol Lab Med 2006; 130:e35
Montgomery EA, Devaney KO, Giordano TJ, et al. Inflammatory myxohyaline tumor of distal extremities with virocyte or Reed-Sternberg-like cells: A distinctive lesion with features simulating inflammatory conditions, Hodgkin’s disease, and various sarcomas. Mod Pathol 1998; 11:384.
Meis-Kindblom JM, Kindblom LG. Acral myxoinflammatory fibroblastic sarcoma: a low grade tumor of the hands and feet. Am J Surg Pathol 1998; 22:911.