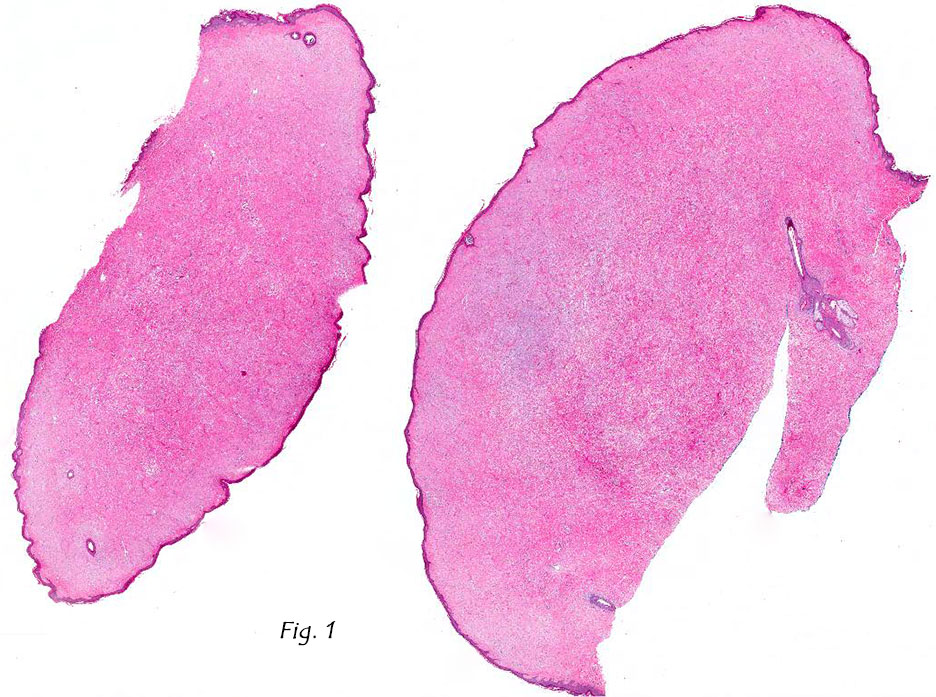
History: A 37-year-old man presented with a well circumscribed, unencapsulated, bluish pink 2.3 x 2.3 cm nodule on his right shin. A 2.0 x 2.0 cm shave biopsy was taken (Fig. 1).
{kind=link}
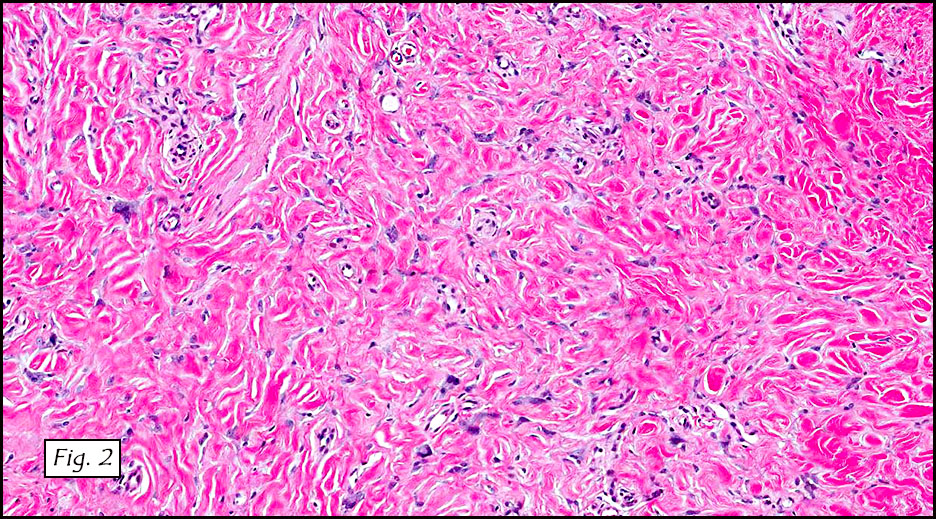
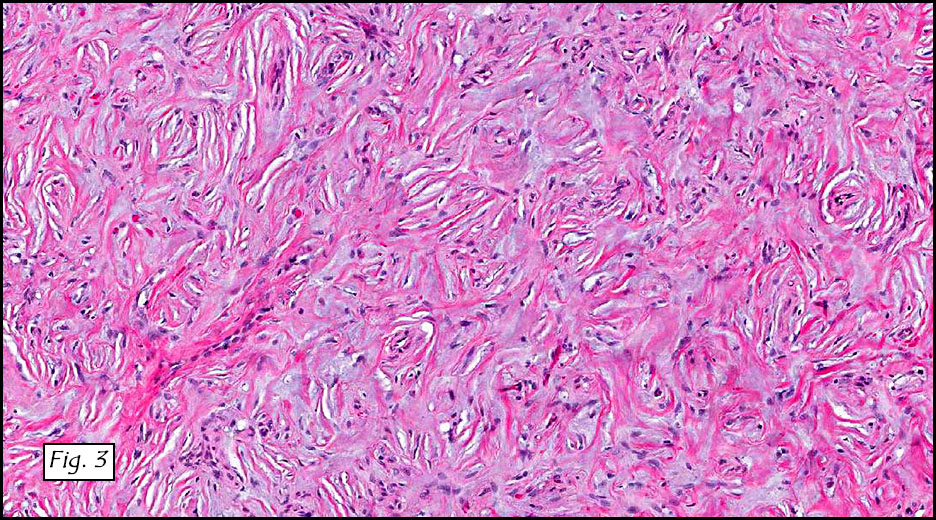
Microscopically, the tumor was dermal-based and involved adnexal structures. It consisted of disorganized collagenous fibers (Fig. 2) admixed with scattered hyperchromatic pleomorphic cells. Myxoid stromal change and storiform patterns were also seen (Fig. 3).
{kind=link}
{kind=link}
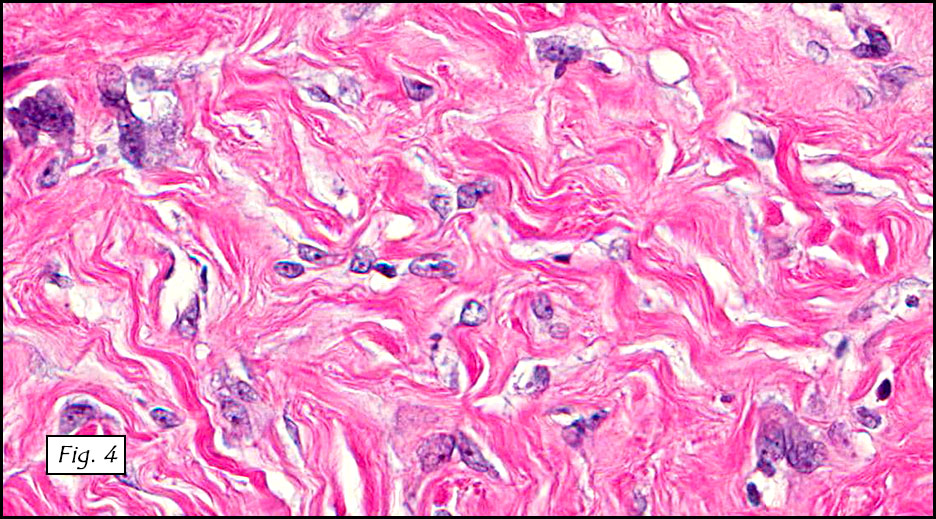
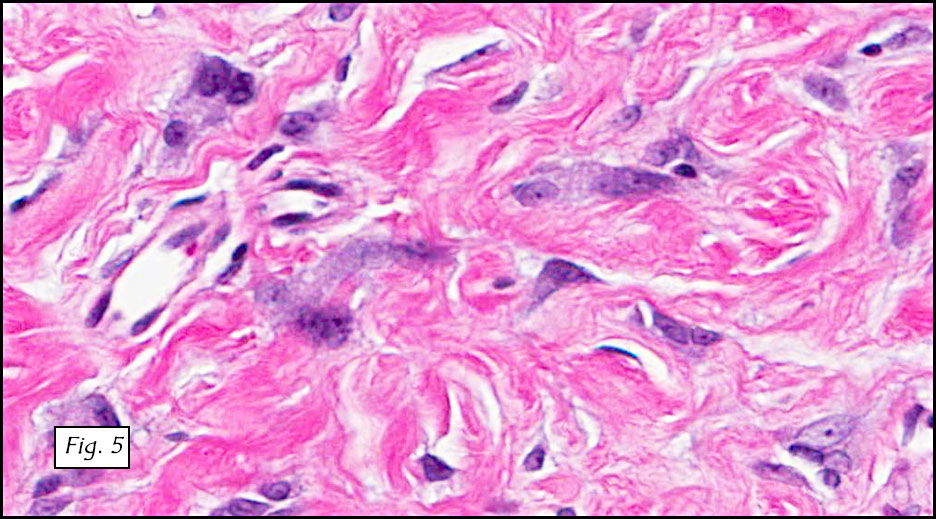
The pleomorphic cells showed enlarged, spindled to stellate-shaped nuclei with small basophilic nucleoli (Fig. 4). These atypical cells showed marked variation in nuclear size and shape. Generally they had indistinct cytoplasmic borders. Many of the more bizarre cells showed enlarged hyperchromatic nuclei (Fig. 5). Multinucleated giant cells with jumbled nuclei were occasionally present. Mast cells, adipocytes, hemosiderin or other pigments were absent. Neither necrosis nor mitotic figures were identified.
{kind=link}
{kind=link}
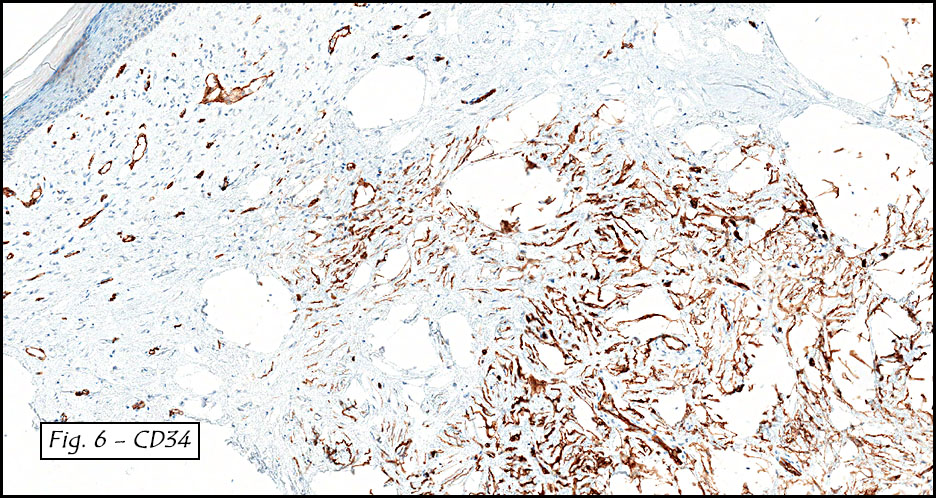
A CD34 stain highlighted the atypical cells, stroma and blood vessels (Fig. 6).
{kind=link}
Diagnosis: Pleomorphic Fibroma of the Skin
Li Lei, M.D., Ph.D., Camilla Cobb, M.D. and Donald R. Chase, M.D.
Department of Pathology and Human Anatomy
Loma Linda University Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Pleomorphic fibroma (PF) of the skin, as its name implies, is a cutaneous lesion characterized by pleomorphic cells in a fibrotic stroma. A lesion of similar morphology may be seen in tendons and has been termed “PF of tendon sheathâ€. PF was first described in 1989 by Dr. Kamino et al. Since then only a handful of cases have been reported. The incidence and prevalence of PF are unclear.
Clinically, PF affects adults in a wide age range (27-75 years) with a median of 50 years. There is a slight predilection for females. No racial difference has been documented. Patients often present with a slowly-growing, solitary, cutaneous nodule usually involving the extremities, followed by the trunk and the head and neck. It is usually asymptomatic but may occasionally be associated with dull pain and/or pruritus. On physical examination, the nodule is small (< 2 cm), polypoid or sessile, and indurated. It is well-circumscribed but non-encapsulated, with a whitish solid firm cut surface.
Histologically, PF is a hypocellular dermal lesion composed predominantly of dense, haphazardly arranged collagen. Interspersed between the collagen fibers are spindle-shaped or stellate cells and focal multinucleated giant cells. The most characteristic feature is degenerative nuclear atypia, presented as large, bizarre, hyperchromatic nuclei with smudged chromatin and small nucleoli. Mitotic figures are rare or absent. Necrosis is not seen. There is minimal inflammatory infiltrate.
Many times the stroma is densely sclerotic, in fact PF may intimately coexist with sclerotic fibroma with a thin transitional area in between. Because of this, the term “Pleomorphic Sclerotic Fibroma†has been suggested as an alternative term which encompasses a proposed spectrum.
It is not uncommon for PF to show focal or diffuse myxoid stromal changes. Although these changes usually lack clinical significance, Dr. Weedon and colleagues reported a case of myxoid PF which transformed into a grade III myxofibrosarcoma.
Immunohistochemically, the cells are strongly positive for vimentin, and variably positive for CD34, smooth muscle actin, muscle-specific actin and CD99. They are negative for CD31, desmin, S-100, CD68 and cytokeratin.
The differential diagnosis of PF includes:
• Atypical fibroxanthoma: This tumor almost always involves sun damaged skin of the elderly and grows rapidly. Histologically, it is hypercellular and composed of spindled to bizarre cells and xanthoma cells. Mitotic figures are brisk and can be atypical. CD10 positivity is seen in 95% of cases. Approximately half of the cases are CD68 positive.
• Dermatofibroma with atypical cells is usually more cellular than PF. Atypical cells are intermixed with spindle cells and histiocyte-like cells. Hemosiderin and siderophages are often present. It is typically CD34 negative. Another helpful tool is pan-monocytic/macrophage marker Ki-M1p which is positive in dermatofibroma with atypical cells but negative in PF.
• Giant cell fibroblastoma usually affects children. The characteristic feature is pseudovascular spaces that are lined by a discontinuous row of CD34 positive atypical spindle cells and floret-like giant cells. Cytogenetic studies show supernumerary ring chromosome derived from t (17; 22).
• Pleomorphic hyalinizing angiectatic tumor can be distinguished by clusters of ectatic thin-walled vessels with fibrin deposition. Pleomorphic stromal cells often contain intracytoplasmic hemosiderin and/or intranuclear pseudoinclusion. A mixed inflammatory infiltrate is usually present in the background.
• Atypical lipomatous tumor (ALT): Normal adipose tissue may occasionally get entrapped in PF, causing diagnostic confusion with dermal ALT. At the molecular level, PF lacks MDM2 amplification by fluorescent in situ hybridization as well as MDM2 protein expression by immunohistochemistry, whereas MDM2 amplification is 93.5% sensitive for diagnosing ALT. Interestingly, Dr. Rosai and Dr. Aguilar reported a case with PF in the dermis and ALT in the contiguous subcutis. Whether or not this is purely coincidental is unclear.
• Pleomorphic lipoma: The typical locations include posterior neck, shoulder and back. The bizarre cells display a wreath-like arrangement of nuclei around deeply eosinophilic cytoplasm, giving them a floret-like appearance. Mast cells are often present. CD 34 is typically positive. Cytogenetic studies show loss of 16q or 13q.
• Ancient schwannoma is usually large and located in deep structures such as the retroperitoneum. Besides nuclear atypia, other degenerative changes including cyst formation, calcification, hemorrhage and hyalinization are also present. Immunostaining for S-100 highlights most of tumor cells. CD34 marks only blood vessels.
• Neurofibroma with nuclear atypia shows isolated mild nuclear. It is usually more cellular than PF and composed of polymorphous proliferation. Collagen fibers have a “shredded carrots†appearance. Mast cells, and occasionally pseudomeissnerian bodies, are present. Immunostaining for S-100 picks up a subset of cells.
• Spindle cell/sarcomatoid squamous cell carcinoma typically occurs on sun-damaged skin of elderly men as a raised, ulcerated nodule. Keratin pearls, connection to epidermis and epidermal lesion are discriminating morphological features. Strong immunoreactivities for both p63 and high molecular weight cytokeratins confirm keratinocytic derivation of tumor cells.
• Desmoplastic melanoma is often deceptively amelanotic with prominent interstitial fibrosis. However, it has a predilection for sun-damaged skin of the elderly, particularly head and neck areas. Morphologically, it can be distinguished by neurotropism, nodular lymphocytic aggregates, lymphovascular invasion and in situ components such as lentigo maligna. Immunohistochemically, though negative for HMB45 and Melan A, it is positive for S-100 and SOX10.
• Desmoplastic fibroblastoma, sometimes referred to as collagenous fibroma, usually arises in deep subcutaneous tissue or skeletal muscle. The scattered spindle or stellate-shaped cells lack atypia and CD34 expression.
The etiology of PF remains unknown. Patients usually report no history of trauma or other stimuli to the area. The immunoprofile of PF suggests origin from myofibroblasts and/or dermal dendrocytes. Cytogenetic and molecular studies are currently sparse.
Nuclear atypia, in the absence of other evidence suggestive of malignancy, is considered a degenerative phenomenon that can be seen in many benign neoplasms including some of the aforementioned as well as non-neoplastic entities such as ischemic fasciitis. It is important to recognize that degenerative atypia does not adversely affect the prognosis. Therefore, over-treatment should be avoided. Simple excision is usually curative for PF, with local recurrences rarely seen in incompletely excised lesions. To the best of our knowledge, metastasis has never been reported.
Suggested Reading:
Goldblum J, Folpe A, Weiss S. Enzinger & Weiss’ Soft Tissue Tumors, 6th ed: Philadelphia, Elsevier Inc, 2014; 216-218.
Brenn T. Pleomorphic dermal neoplasms: a review. Adv Anat Pathol. 2014;21:108-30.
Al-Zaid T, Wang WL, Lopez-Terrada D, Lev D, Hornick JL, Hafeez Diwan A, Fletcher CD, Lazar AJ. Pleomorphic fibroma and dermal atypical lipomatous tumor: are they related? J Cutan Pathol. 2013;40:379-84.
Aguilar C, Rosai J. Pleomorphic fibroma of the skin, atypical lipomatous tumor, or both? Int J Surg Pathol. 2011;19:63.
Dore A, Robertson I, Williamson R, Weedon D. Progression of a myxoid pleomorphic fibroma to myxofibrosarcoma. Australas J Dermatol. 2003;44:287-90.
Rudolph P, Schubert C, Zelger BG, Zelger B, Parwaresch R. Differential expression of CD34 and Ki-M1p in pleomorphic fibroma and dermatofibroma with monster cells. Am J Dermatopathol. 1999;21:414-9.