 History: An 82 year old woman presented with multiple nodules in the left breast eight months following local resection of a cutaneous angiosarcoma in the same breast. A simple mastectomy was performed but she died the following day due to cardiac complications.
History: An 82 year old woman presented with multiple nodules in the left breast eight months following local resection of a cutaneous angiosarcoma in the same breast. A simple mastectomy was performed but she died the following day due to cardiac complications.
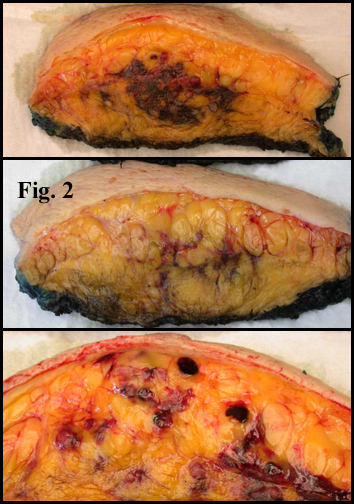
Gross examination of the 1145 gram, 27.0 x 20.0 x 4.0 cm mastectomy specimen showed a 10.0 x 5.0 x 2.0 cm hemorrhagic neoplasm involving the central and lateral regions. It closely approached the overlying skin (Figs. 1, 2).
{kind=link}
{kind=link}
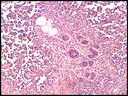
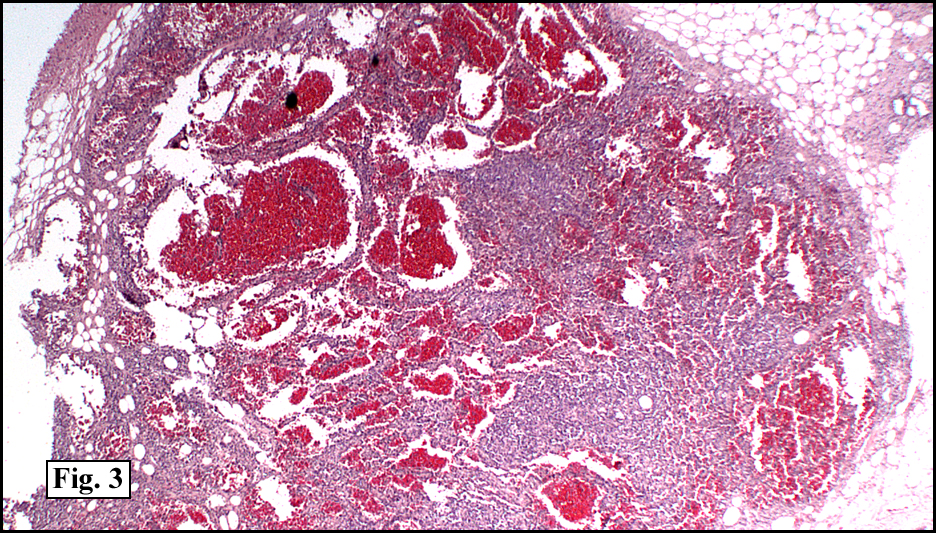
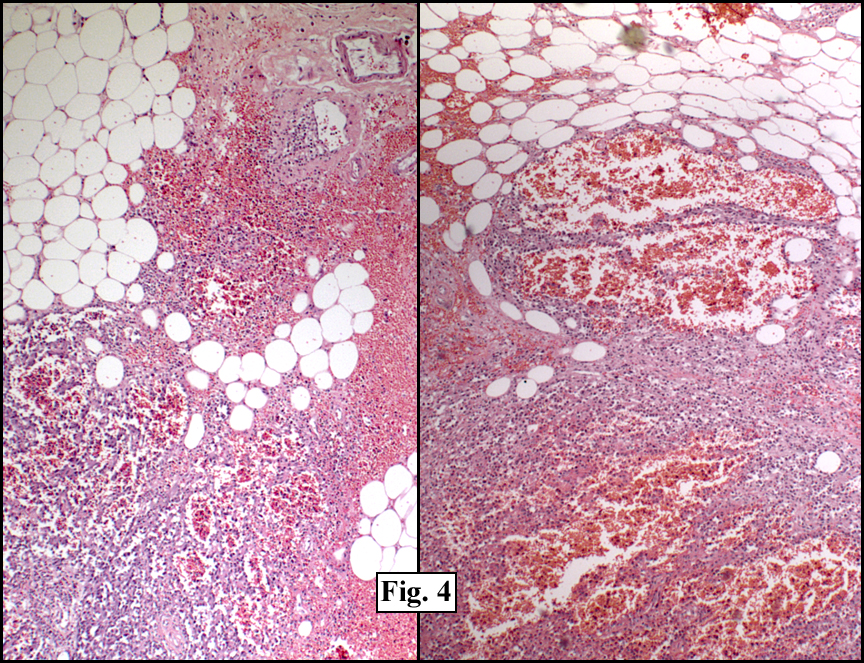
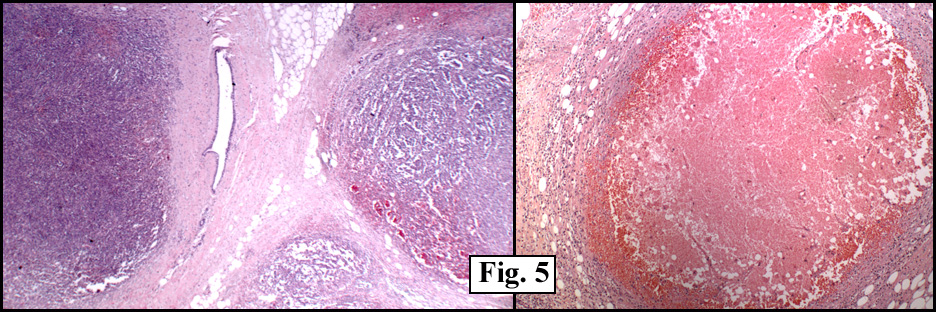
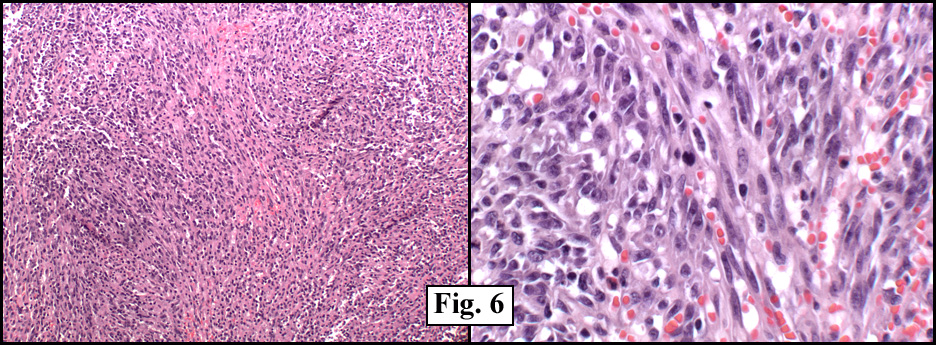
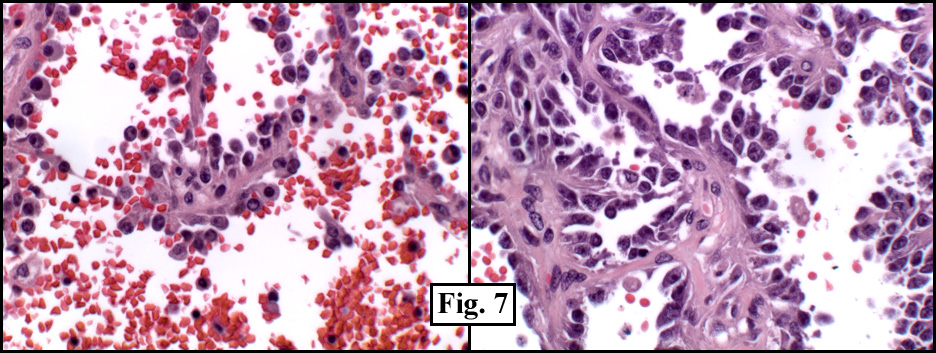
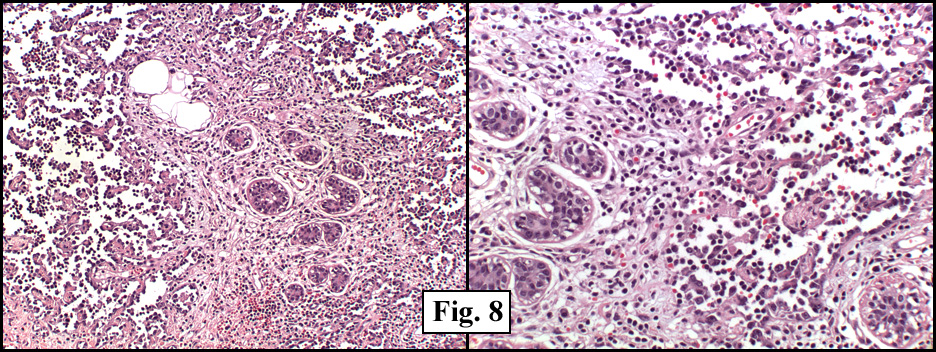
Microscopic sections revealed a vascular neoplasm with dilated spaces filled with erythrocytes (Fig. 3). The tumor was infiltrative into fat (Fig. 4) and had a marked nodular growth pattern with areas of necrosis (Fig. 5). There were solid areas which lacked vascular spaces that consisted of spindled cells and extravagated blood cells resembling Kaposi’s sarcoma (Fig. 6). Other regions showed irregular spaces lined by polygonal cells with prominent nucleoli (Fig. 7). The tumor infiltrated native breast ductal and lobular elements (Fig. 8). Occasional mitoses and areas of necrosis were present (Figs. 5, 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Angiosarcoma of the Breastâ€
Michelle Fajardo DO, Mark Janssen MD, Donald R. Chase MD
Department of Pathology, Loma Linda University and Medical Center
California Tumor Tissue Registry
Discussion: Mammary angiosarcoma (AS) is an aggressive vascular neoplasm first described in 1887. It generally occurs in the fourth to fifth decade almost exclusively in the female breast. Although it is the most common sarcoma of the breast, the tumor is exceptionally rare, comprising 0.04% of primary breast tumors and 8% of breast sarcomas. Clinically, the lesion presents as a rapidly growing, painless, discrete mass. Unlike mammary carcinomas, nipple retraction, discharge, and axillary lymphadenopathy are generally absent.
AS is usually spongy or friable in consistency with hemorrhagic areas and poorly defined margins. It consists of atypical endothelial cells lining aberrant vascular spaces which are variably filled with erythrocytes. The tumor is usually divided into three groups:
• Grade I (well differentiated) lesions show well-formed vascular channels with one to two layers of endothelial cells. Papillary growth and endothelial tufting are minimal to absent. Mitoses are rare. Hemorrhage, necrosis, and pleomorphism are not generally present.
• Grade II (moderately differentiated) tumors are characterized by irregular vascular channels with papillary growth and endothelial tufting. There may be focal solid areas composed of spindled cells. Mitoses are present, but necrosis is usually absent.
• Grade III (poorly differentiated) lesions consist of predominantly solid areas of malignant polygonal or spindled cells. Few well-developed vascular channels are present but may be difficult to identify. Mitotic figures, hemorrhage, necrosis, and pleomorphism are common findings.
Vascular markers CD31 and CD34 show variable staining. Well-differentiated tumors may stain positive with Factor VIII antigen and/or Ulex europaeus. Although not generally performed, electron microscopy may show classic Weibel-Palade bodies in the atypical endothelial cells.
The differential diagnosis of mammary AS can be extensive due to the spectrum of morphologic patterns that the tumor may assume. It may closely mimic spindle cell lesions including Kaposi’s sarcoma as well as other vascular tumors. But a hallmark of the tumor is its infiltration of native structures and fat. Aberrant vascular spaces characteristically intersect adipose tissue and separate lobular units from their “feeding†ducts. In general, the three main mimics are:
• Mammary hemangioma is a common vascular lesion that is well-defined and has a distinct lobular pattern. The endothelial cells are uniform, without atypia. Infiltration between native structures does not occur.
• Angiolipoma is a painful, sharply demarcated tumor characterized by a proliferation of vascular channels with microthrombi and mature adipocytes. Mitotic figures are not seen and neither necrosis nor hemorrhage are encountered.
• Angiomatosis shows a uniform pattern of cytologically bland vessels which lack papillae or tufting.
AS of the breast is a highly aggressive tumor with a poor prognosis. Metastasis occurs to the lungs, liver, skin, bones, contralateral breast, and less often to the ovary or spleen. Unlike AS in other sites, studies have shown that a higher survival rate in mammary AS correlates with histologic grade, with Grade I lesions having the best prognosis. Because prognosis is related to tumor grade, the lesion should be extensively sampled in order to establish the tumor type.
Treatment of AS consists of total mastectomy generally without axillary lymph node dissection since metastasis to nodes is rare. Dactinomycin shows some success in limiting recurrence in Grade III lesions, but has not been shown to be effective in Grade I or II tumors.
Suggested Reading:
Farrokh D, Hashemi J, Zandi B. Angiosarcoma of the breast: Report of a case and literature review. Iran J Radiol 3(2): 81-84, 2006.
Ohta M, Tokuda Y, Kuge S, Okumura A, Tanaka M, Kubota M et al. A case of angiosarcoma of the breast. Japanese Journal of Clinical Oncology 27 (2): 91-95, 1997.
Rosen PP, Kimmel M, Ernsberger D. Mammary angiosarcoma: The prognostic significance of tumor differentiation. Cancer 62(10):2145-2151, 1988.
Silverman LR, Deligdisch L, Mandeli J, Greenspan EM. Chemotherapy for angiosarcoma of the breast: Case report of 30-year survival and analysis of the literature. Cancer Invest 12(2): 145-155.
Tavassoli F. Pathology of the Breast, 2nd Ed. Appleton and Lange: Stamford, Connecticut, 1999.
Weiss SW, Enzinger FM. Soft Tissue Tumors, 4th Ed. Mosby Inc.: St. Louis, MO, 2001.