 History: A 41 year-old man presented in orthopedics clinic with a complaint of a slow-growing mass in his left calf. The patient was a long-haul trucker who stated that he first began to notice a gradual enlargement of his calf following minor trauma sustained while falling off his truck. He complained of a moderate amount of aching pain (rated 2-3/10 in intensity) without radiation. He indicated that the pain was not made worse with activity and was intensely felt with flexion of the knee.
History: A 41 year-old man presented in orthopedics clinic with a complaint of a slow-growing mass in his left calf. The patient was a long-haul trucker who stated that he first began to notice a gradual enlargement of his calf following minor trauma sustained while falling off his truck. He complained of a moderate amount of aching pain (rated 2-3/10 in intensity) without radiation. He indicated that the pain was not made worse with activity and was intensely felt with flexion of the knee.
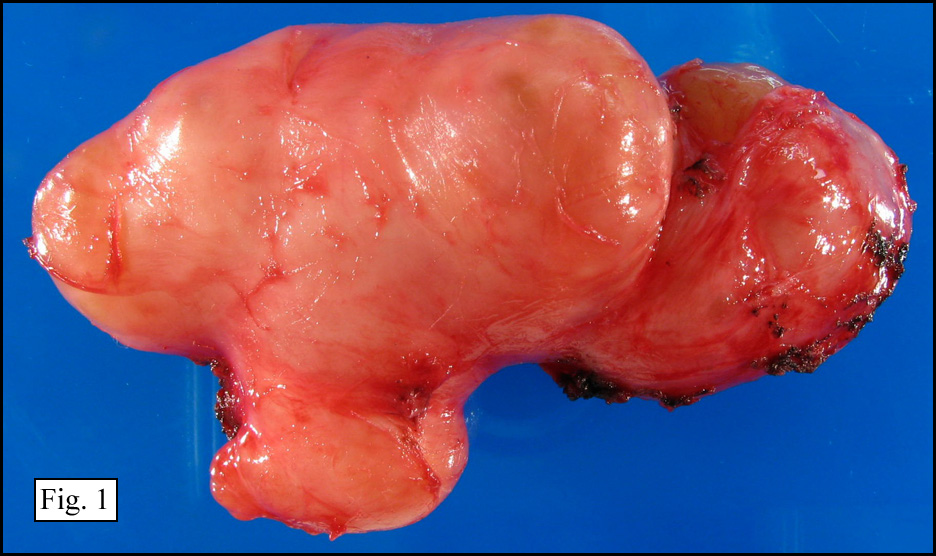
A mass was palpated at the mid-substance of his gastroc-soleus complex of the left calf. At surgery, an 11.0 x 4.5 x 4.3 cm well-circumscribed lobulated soft tissue mass with a pink-white fibrous capsule surrounding fleshy yellow-tan to pink parenchyma was removed from the patient’s left popliteal fossa (Figs. 1,2). The surgeon thought that it arose from the nerves at the level of the trifurcation.
{kind=link}
{kind=link}
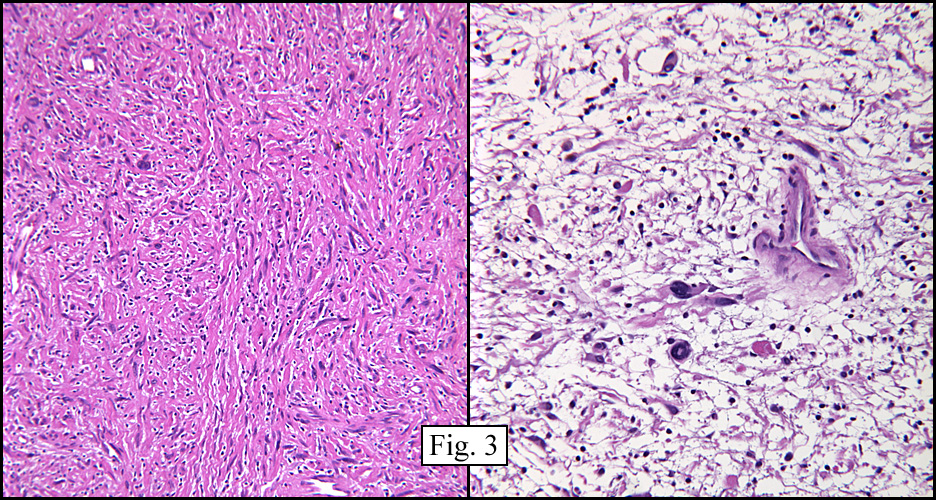
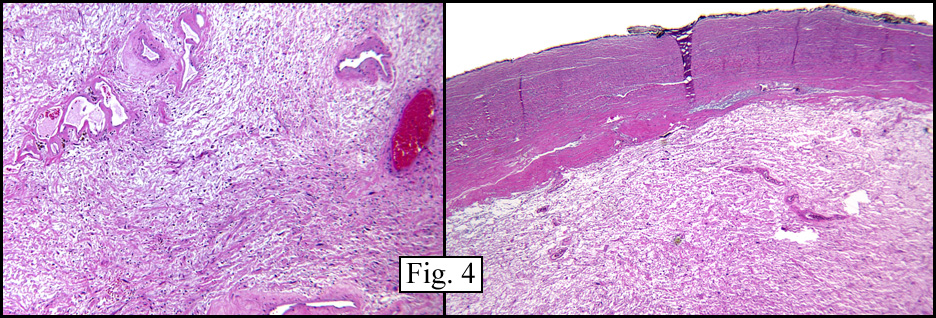
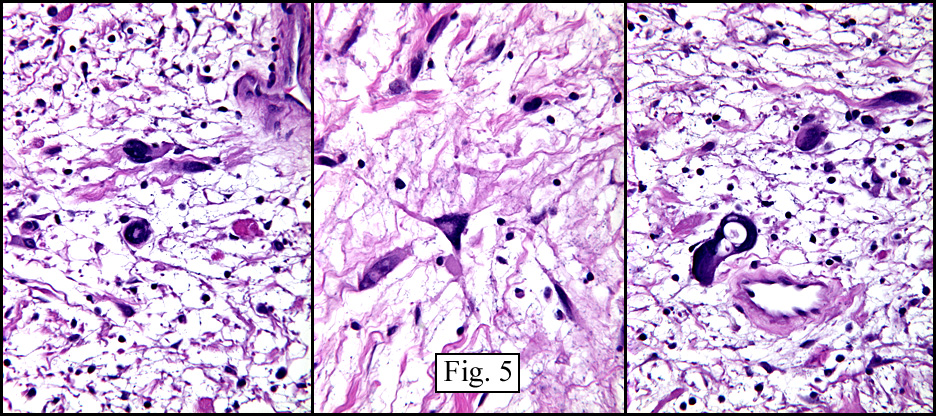
Sections showed a spindle cell lesion of varying cellularity with both densely packed areas and looser areas and having a myxoid background (Figs. 3,4). Hyalinized blood vessels, some with developing thrombi, were seen throughout the lesion (Fig. 5). The mass was well circumscribed and surrounded by a thick fibrous capsule. Intermixed with benign-appearing spindle cells were large cells with striking atypia.
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Ancient Schwannoma†(‘Schwannoma with degenerative atypia’)
Melissa Sakaugset PSF, Donald R. Chase MD
Department of Pathology, Loma Linda University and Medical Center
California Tumor Tissue Registry
Discussion: This benign variant of schwannoma is distinguished by marked degenerative nuclear atypia. It is thought that this worrisome change is degenerative in nature and likely secondary to the extremely slow growth of the lesion. One study showed a mean interval between onset of symptoms and surgical resection of 8.3 years with a range of 1-20 years.
Ancient Schwannoma (AS) is a well-circumscribed soft tissue mass usually in close association with a nerve (often reported either radiologically and/or surgically) that can have degenerative changes including calcification, cyst formation, hyalinization, and hemorrhage. Calcification is quite common. Microscopically, the Schwann cells may be very atypical with large hyperchromatic, often multi-lobed, nuclei with coarsely clumped chromatin. A large degree of pleomorphism is often seen. AS is usually mitotically “inertâ€, showing no mitotic activity and little or no proliferative activity by immunostains.
When evaluating a slow-growing soft tissue mass it is important to consider the diagnosis of AS. Although cytologic preparations may show atypia suggesting malignancy, the radiologic findings are helpful, uniformly showing a well-circumbscribed mass without invasive characteristics. The complete lack of mitotic activity is also important and helps to exclude MFH, which shows both cellular pleomorphism and mitotic activity.
While AS usually has a biphasic pattern of Antoni A and B areas some tumors may have near absence of hypercellular Antoni A. In the presence of the pleomorphism and nuclear atypia this can pose a diagnostic challenge. In this setting immunohistochemistry is particularly helpful. AS consistently decorates with S100 in the same manner as do typical schwannomas. The pattern is diffusely and strongly positive with both nuclear and cytoplasmic staining. In addition, the Schwann cells may also be GFAP positive.
Physical examination and imaging studies may be of considerable help. AS tends to present as a palpable mass with a long clinical course. Local pain is often present and in some cases, radiating pain can be elicited by tapping on the tumor (Tinel’s sign). Features rendering it distinct from its radiologic mimics (MFH, MPNST, liposarcoma, synovial sarcoma, and HPC) include visualization of an adjacent nerve, a rim of fibrous capsule, and circumferential degeneration and calcification.
Ancient Schwannomas are benign tumors with virtually no risk of local recurrence. Accurate diagnosis is critical in preventing more extensive resections usually necessitated in malignancies that it mimics. Recognition of this “atypical†proliferation as being benign is key in proper patient care.
Follow-up: The patient did well post-excision. He had some sensory deficit to sharp/dull sensation in the distribution of the sural nerve, but required no additional treatment. The tumor has not recurred and he has resumed normal functions.
Suggested Reading:
Fletcher, CDM. Diagnostic Histopathology of Tumors, 2nd ed. Churchill Livingstone, 2000.
Isobe, K, Shimizu T, Akahane T, Kato H. Imaging of Ancient Schwannoma. Am J Roent 183: 331-336, 2004.
Miettinen, Markku, MD. Diagnostic Soft Tissue Pathology. Churchill Livingstone, 2003.
Strouhal, Eugen; Nemeckova, Alena. Paleopathological Find of a Sacral Neurilemmoma From Ancient Egypt. Am J Physical Anthropol 125: 320-328, 2004.
Weiss, Sharon W, Goldlum, JR. Enzinger and Weiss’s Soft Tissue Tumors, 4th ed Mosby, inc, 2001.