History: A 35-year-old woman presented with persistent post-coital bleeding. Examination revealed a coarsely granular, tan mass protruding from the cervical os. Following multiple cervical biopsies, the patient underwent a hysterectomy with bilateral salpingo-oophorectomy. A 6.6 x 2.5 x 0.8 cm well-circumbscribed, exophytic tumor was removed from the region of the transition zone.
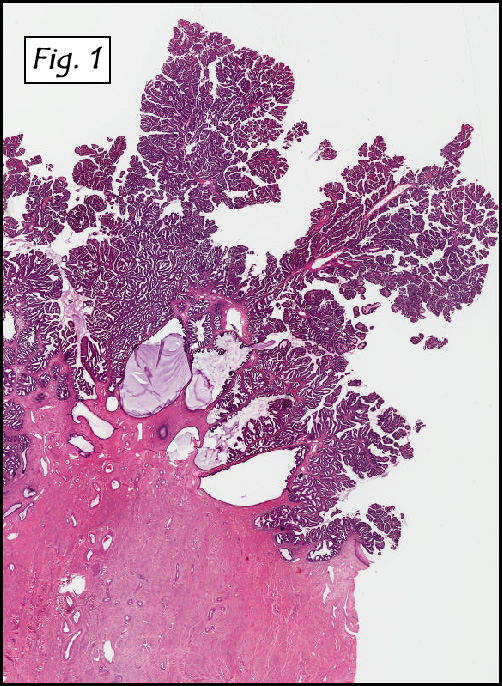
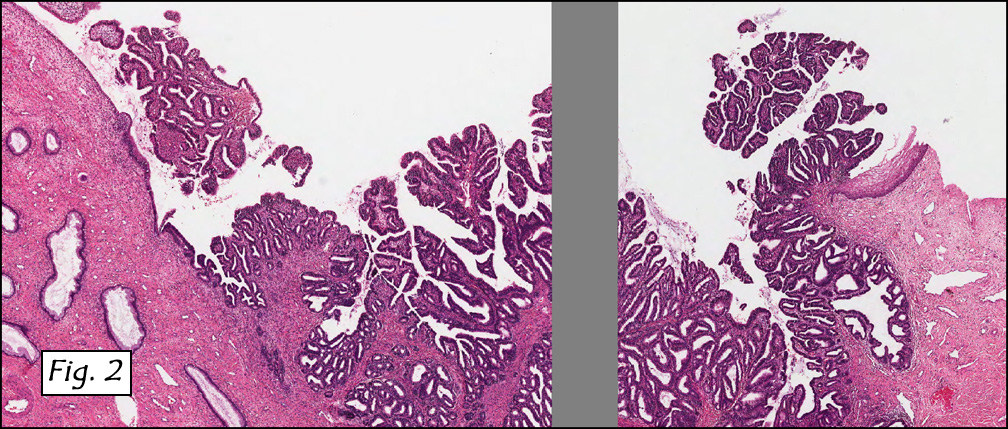
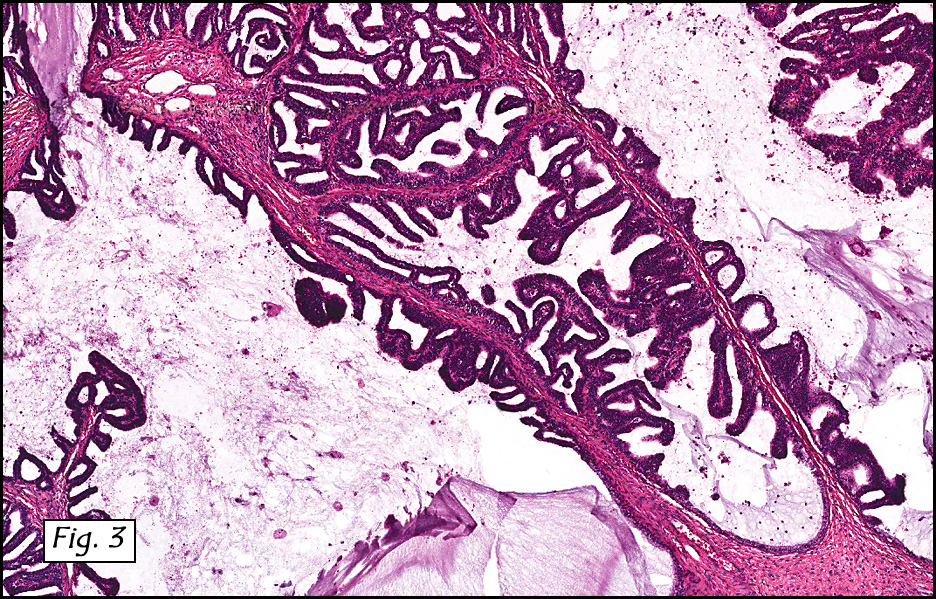
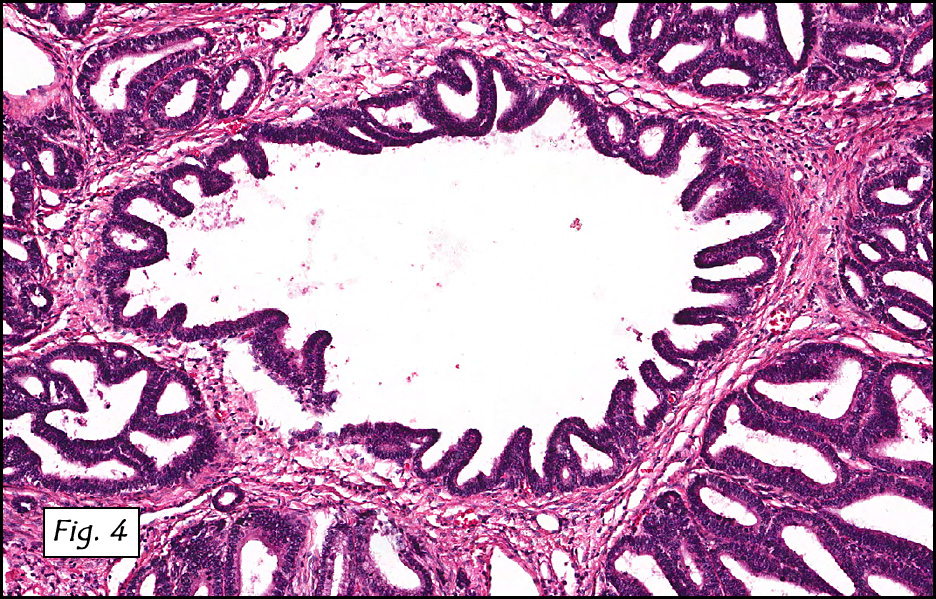
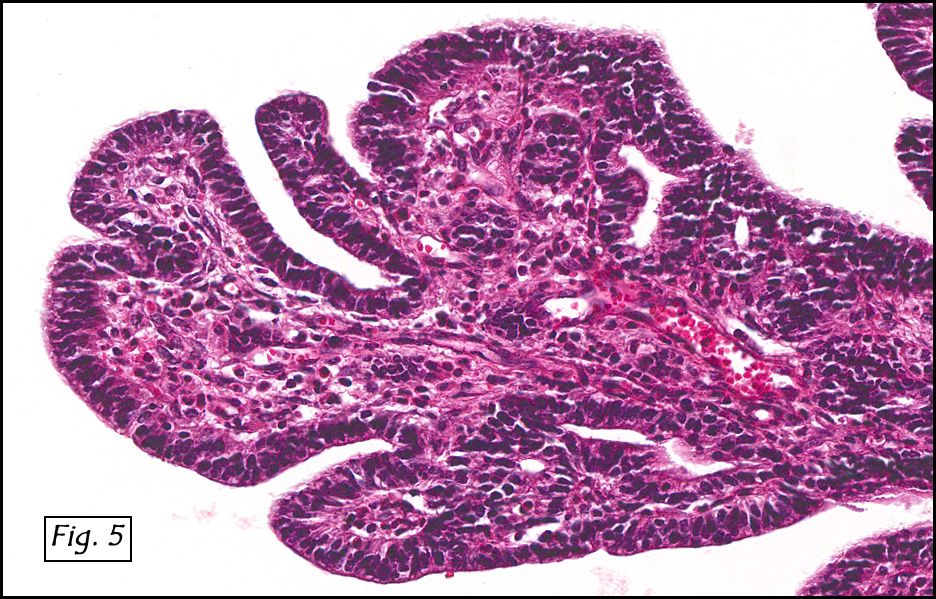
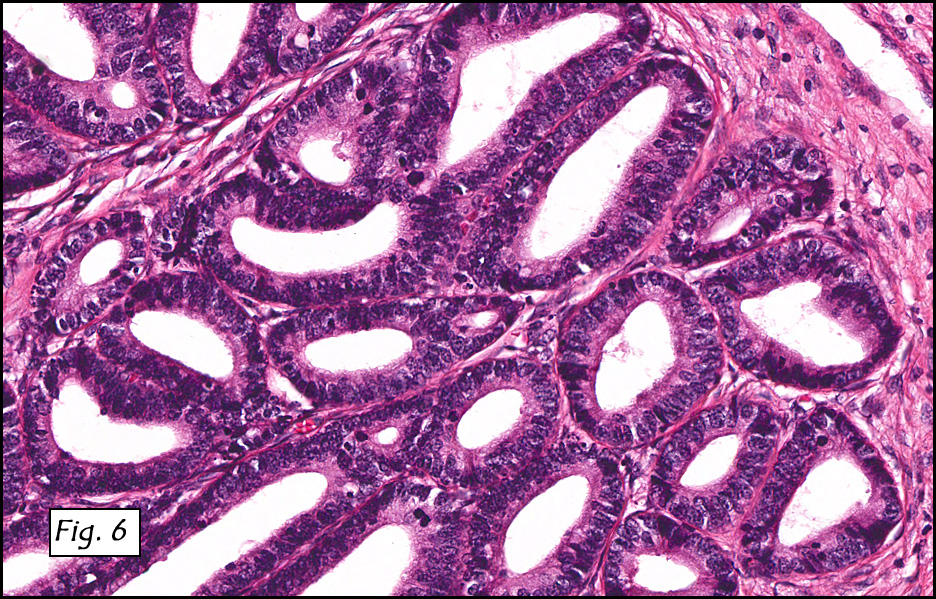
Microscopically, the mass was mostly exophytic (Fig. 1), involved the squamo-columnar junction (Fig. 2), and only superficially invaded the underlining cervical tissue. It was uniformly papillary with long thin branching papillae that were lined by endocervical-type epithelium. Occasional mucin-filled cysts were present at the base (Fig. 3). The lining cells showed minimal cytologic atypia and displayed mild nuclear stratification. Although papillary and micropapillary regions dominated (fig. 4), some areas were “adenomatous†resembling tubular adenomas of the colon. Most of the cells had abundant eosinophilic cytoplasm and had nuclei with finely granular chromatin and small but distinct nucleoli (Fig. 5, 6). Occasional cells showed discrete vacuoles, suggestive of some degree of mucinous differentiation. Mitotic figures were rarely seen. Neither lymphovascular nor perineural invasion was present.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Well Differentiated Papillary Adenocarcinoma of Cervix / Villoglandular Adenocarcinomaâ€
Jin Guo, MD, and Donald R. Chase, MD
Department of Pathology, Loma Linda University and Medical Center,
Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: First reported in 1989, villoglandular adenocarcinoma (VGA) is a rare tumor of the uterine cervix with just over 100 cases in the literature. It mostly arises in young women (often <40 years) without known risk factors. Patients usually present with vaginal bleeding and/or abnormal cervical smears. Although VGA generally carries a good long-term prognosis, it may be locally invasive. There are also scattered reports of metastases and rarely death from the tumor. VGA may be grossly visualized during pelvic examination as an exophytic polypoid cervical mass. It grows as complex papillae varying from long, delicate, fingerlike projections to short, broad, complex and branching excrescences. The fibrovascular cores are covered with stratified endocervical, endometrial or intestinal-type tall columnar epithelium. Generally, the cells have abundant eosinophilic cytoplasm and elongated hyperchromatic mildly atypical nuclei. Mucin production is variable. The deeper regions of the papillae may show adenocarcinoma in situ or superficial invasion. Interpretation of an initial, superficial biopsy is often challenging largely because the tumor usually lacks host desmoplasia, shows minimal atypia, and only occasionally shows invasion. For these reasons deferment of the diagnosis is suggested pending full examination of a cone biopsy or hysterectomy specimen. VGA, having a relatively good prognosis, needs to be distinguished from several conditions including cervical implant(s) from conventional or papillary endometrial adenocarcinoma, serous papillary adenocarcinoma of the cervix, as well as hyperplastic reactive glands. Unlike most endometrial adenocarcinomas, VGA occurs mainly in young women at the cervical transitional zone, and may decorate for HPV. Traditional endometrial adenocarcinomas usually arise in the uterine fundus or ovaries of postmenopausal women and tend to be HPV negative. Serous papillary adenocarcinoma (SPA) of the cervix is rare and resembles serous papillary carcinoma of the ovary or endometrium. Although the growth patterns of SPA and VGA are similar, SPA is less glandular, rarely displays mucinous differentiation, and is highly invasive of both stroma and lymphatics. Unlike VGA, SPA may present with distant metastasis to pelvic and/or periaortic lymph nodes. There is also more cytologic atypia and increased mitotic activity. Reactive, hyperplastic glands do not show the profound villoglandular architecture and lack the degree of cellular atypia of VGA or SPA. VGA usually marks positively for B72.3, Ca-125, carcinoembryonic antigen, keratin 7, and p16 protein. It is usually negative for vimentin, P53, and estrogen and progesterone receptors. Molecular studies with PCR amplification of tumor DNA may reveal a positive signal for HPV-DNA but not for HSV-DNA. Villoglandular adenocarcinoma of the cervix is usually suspected by microscopic examination of tissues from a cervical biopsy and/or a cervical cone. Careful review of this material will show if any further surgery is needed. A completion hysterectomy is usually reserved for residual/recurrent disease, or in those cases showing unequivocal adenocarcinoma, significant invasion, atypical squamous features, and/or high grade glandular dysplasia. Cone biopsy is curative in most cases and also gives the potential benefit of preserving fertility. Suggested reading:
R.H. Young and R.E. Scully. Villoglandular papillary adenocarcinoma of the uterine cervix. A clinicopathologic analysis of 13 cases, Cancer, 63:1773–1779, 1989.
Heather Stanley-Christian, Bradley K. Heim, Jeffrey F. Hines, Kevin L. Hall, Gerald D. Willett and Willard A. Barnes. Villoglandular Adenocarcinoma of the Cervix: A Report of Three Cases and Review of the Literature. Gyn Oncol, 66(2):327-330, 1997.
R.D. Macdonald, J. Kirwan, K. Hayat, C.S. Herrington and H. Shawki. Villoglandular adenocarcinoma of the cervix: Clarity is needed on the histological definition for this difficult diagnosis. Gyn Oncol 100(1):192-194, 2006.
Michael S. Ballo, M.D., Steven G. Silverberg, M.D., and Mary K. Sidawy, M.D. Cytologic Features of Well-Differentiated Villoglandular Adenocarcinoma of the Cervix. Acta Cytol, 40:536-540, 1996.
Fadare Oluwole, Wenxin Zheng. Well-differentiated papillary villoglandular adenocarcinoma of the uterine cervix with a focal high-grade component: is there a need for reassessment? Virch Archiv, 447:883-887, 2005.
Giovanna Giordano, Tizsiana D’Adda, Letizia Gnetti, Carla Merisio, Marzio Gabrielli, Mauro Melpignano. Villoglandular adenocarcinoma of the cervix: two new cases with morphological and molecular study. Int J Gynecol Pathol, 26(2):199-204, 2007.
Richard J Zaino M.D. Glandular Lesions of the Uterine Cervix. Mod Pathol, 13(3):261-274, 2000
Young RH, Scully RE. Villoglandular papillary adenocarcinoma of the uterine cervix: a clinicopathologic analysis of 13 cases. Cancer, 63(9):1773–1779, 1989.
Al-Nafussi A, Obafunwa J, Jordan LB, Fulton I, Martin C, Beattie G. Cervical implant from villoglandular endometrial adenocarcinoma masquerading as cervical villoglandular adenocarcinoma. Int J Gynecol Cancer, 12(3):308-11, 2002.