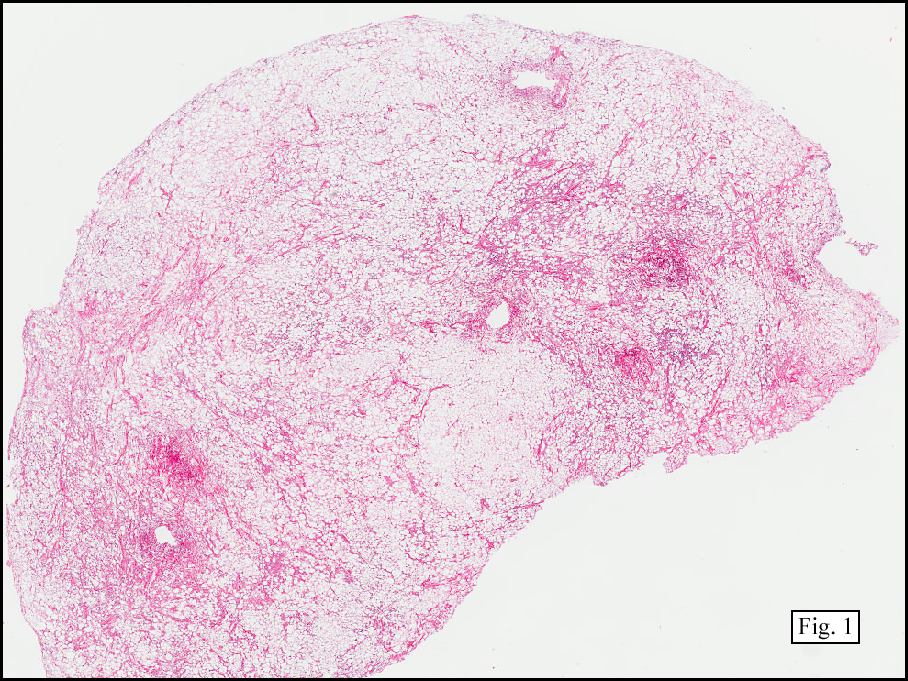
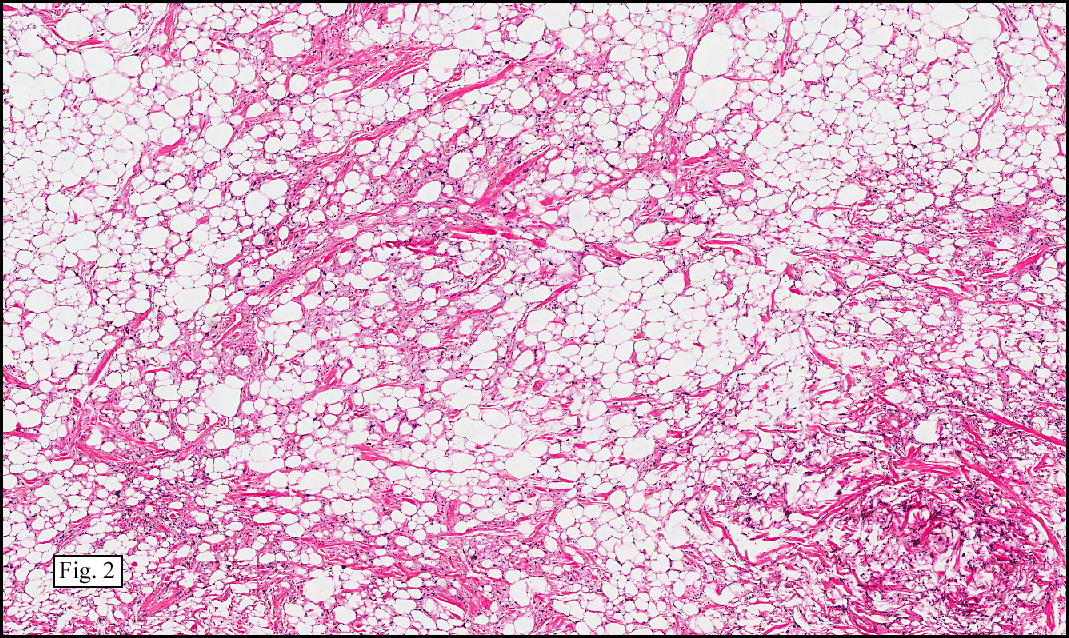
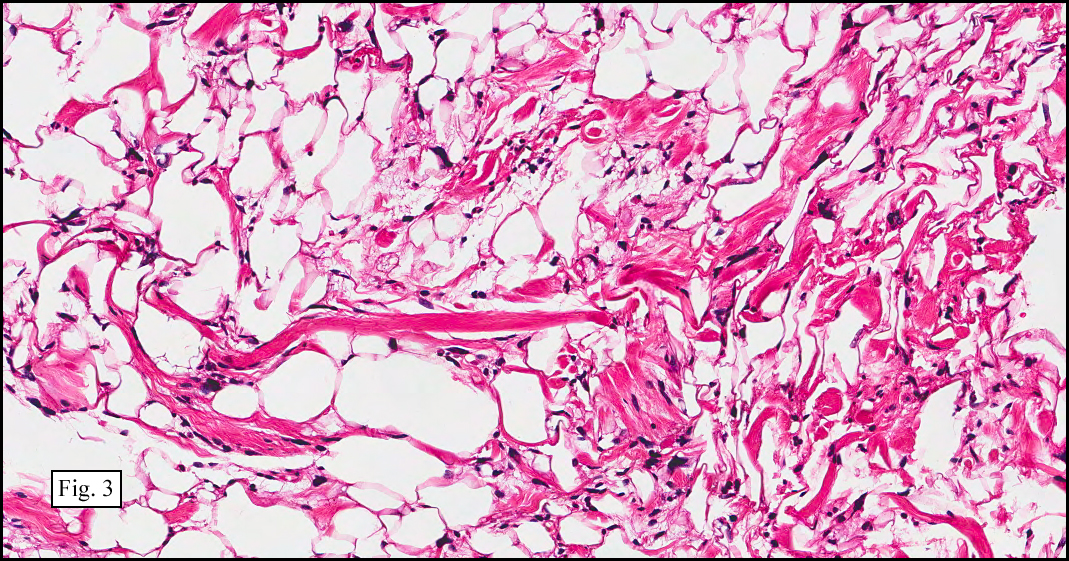
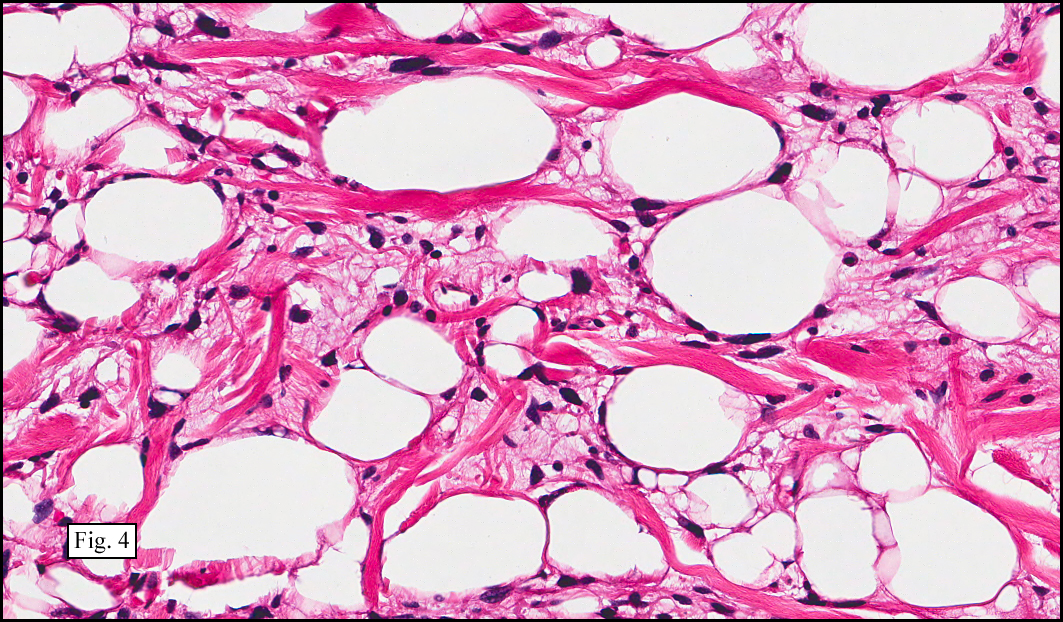
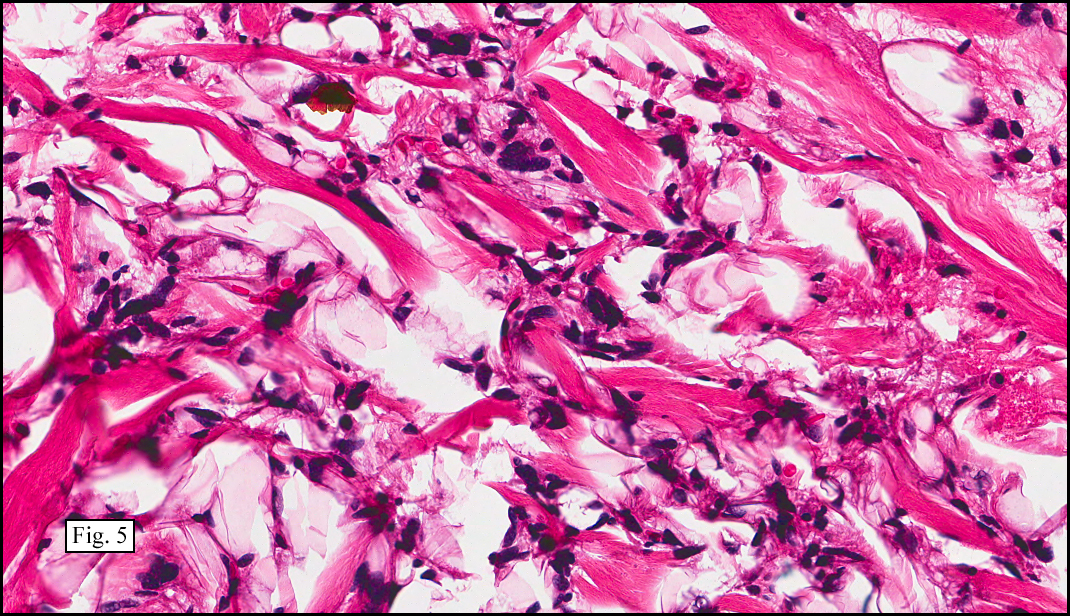
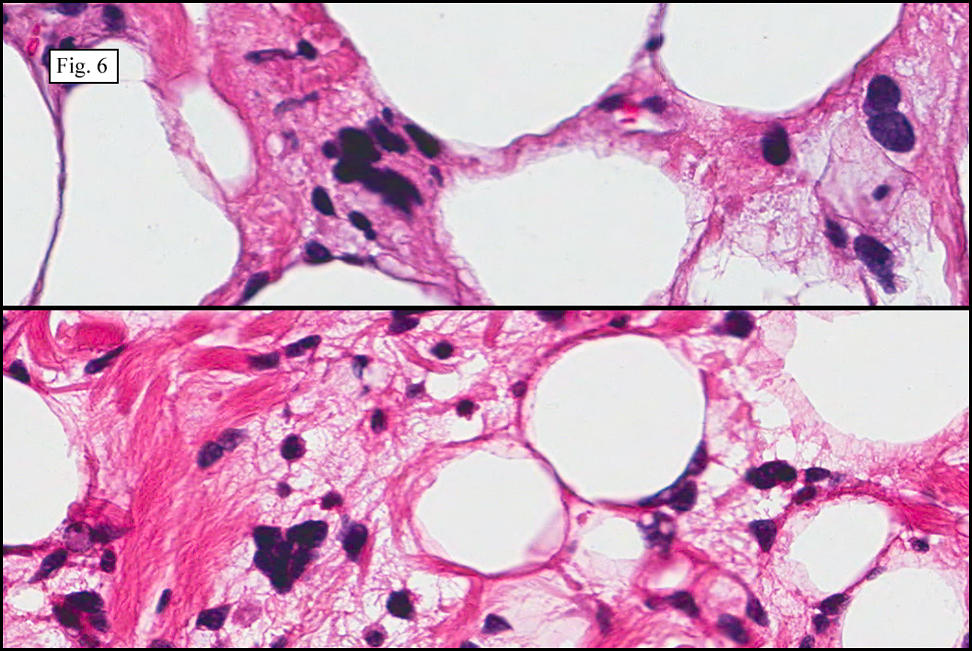
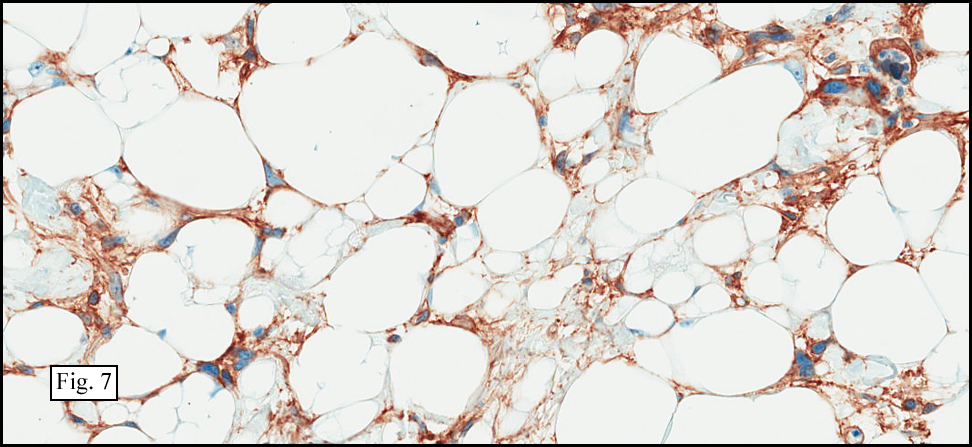
History: A 75-year-old man underwent surgical excision of a 4 x 3 cm yellow-tan, ovoid, lobular and encapsulated right posterior neck mass. It was superficial, approaching to within 1.2 cm of the skin surface. The mass had a homogeneous cut surface and was well circumbscribed (Fig. 1). Mature fat occupied about 50% of the tumor, with the remainder consisting of spindled and pleomorphic cells (Fig. 2). Conspicuous thick bands of eosinophilic, ropey collagen dissected throughout the fat and hyperchromatic spindled cells (Fig. 3, 4). Some areas showed clumping of the atypical spindled cells (Fig. 5). There were also scattered multinucleated giant cells with a “floret-like†appearance (Fig. 6). Neither necrosis nor hemorrhage was seen. Mitotic figures were absent. The tumor strongly decorated for CD34 in both the spindled cells, and the floret elements (Fig. 7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Spindle Cell Lipoma/Pleomorphic Lipoma, Right Posterior Neckâ€
Marnelli A. Bautista, MD, and Donald R. Chase, MD
Department of Pathology & California Tumor Tissue Registry
Loma Linda University and Medical Center, Loma Linda, California
Discussion: Spindle Cell Lipoma (SCL) and Pleomorphic Lipoma (PL) have been recently re-classified as a single entity (SCL/PL) due to their overlapping clinical, cellular, immunoperoxidase and cytogenetic characteristics. They occur mostly in men (85-90%) between the ages of 45-60. Although SCL/PL can occur at other ages, they virtually do not occur before the age of 20. Approximately 80% arise in the posterior neck, shoulder or back, and are virtually always superficial, generally involving subcutaneous tissues. Deeper forms, however, have been described in a variety of sites.
The tumors show a wide histologic spectrum ranging from pure spindle cell lipoma to pure pleomorphic lipoma. Although the fatty component is mostly mature, occasional lipoblast-like cells may also be encountered. Problematically, cases with very minimal to absent adipose tissue have been reported, posing a diagnostic challenge.
In classic SCL, there is relatively equal distribution of mature fat and uniform, bland spindle cells, many of which have hyperchromatic nuclei. The spindle cells may be randomly arranged, clumped, or assembled in short parallel bundles. A consistent finding is eosinophilic, dense or ropey collagen strands admixed with the spindle cells. A pseudoangiomatous variant of SCL has also been described consisting of short bundles of spindle cells partitioned by dense connective tissue projections.
Pleomorphic lipoma also has ropey collagen bundles and occasional spindle cells, but is distinguished by the presence of peculiar giant cells with floret-like nuclear configurations, where the coalescing nuclei are organized into a wreath-like pattern. The spindle cells and floret giant cells stain strongly positive for CD34 but are negative for desmin, actin, keratin and S-100. Mast cells are seen in most cases. Some lesions may also display myxomatous change. On rare occasions, small foci of cartilaginous or osseous metaplasia may be identified. However, mitotic figures are not increased, and atypical forms are rarely present. SCL/PL behaves in a benign fashion, with a very low rate of recurrence once completely excised.
Cytogenetic findings: Most SC/PL show loss of 16q and occasional cases demonstrate loss of 13q, further highlighting the relationship between the two lesions. The absence of ring chromosomes and giant marker helps to separate SCL/PL from atypical lipomatous tumor/well-differentiated liposarcoma (ALT/WDL).
Differential Diagnosis:
• ALT/WDL, particularly the sclerosing type: These tumors are typically located in the deep muscles of the extremities and retroperitoneum. Floret-like giant cells may be encountered, with occasionally scattered atypical or pleomorphic lipoblasts, and dense fibrous zones, but the conspicuous ropey collagen bundles are not usually seen. Also, in contrast to SCL/PL, ALT/WDL is characterized by the presence of giant marker and ring chromosomes.
• Dedifferentiated Liposarcoma (DLS): Greater than 80% of DLS arises in the retroperitoneum. Most areas appear histologically similar to ALT/WDL, with focal overgrowth of pleomorphic sarcoma (dedifferentiation). An abrupt transition between the two regions is usually depicted. The dedifferentiated zone may show little pleomorphism mimicking fibrosarcoma or leiomyosarcoma, but much more commonly has the phenotype of so-called malignant fibrous histiocytoma (pleomorphic sarcoma). As in PL, scattered cells may have floret-like giant cells.
• Pleomorphic Liposarcoma: This least common type of liposarcoma (15%) is deeply located and consists of numerous pleomorphic lipoblasts and on occasion, large, bizarre giant cells. Unlike SCL/PL, the tumor is negative for CD34. Mitotic figures, including atypical forms, are commonly seen.
• Dermatofibrosarcoma Protuberans (DFSP) usually arises superficially within the dermis and infiltrates the underlying subcutaneous tissue. The uniform spindle cells are arranged in a storiform pattern. Giant cells may be encountered in some cases; however, ropey collagen bundles are typically absent, and the process is CD34 negative.
• Giant Cell Fibroblastoma (GCF) is commonly seen in children, usually 3-5 years old. It has been suggested that this lesion represents a juvenile form of DFSP. Multinucleated giant cells, which line the characteristic pseudovascular spaces, may emulate the floret-like giant cells of SCL/PL. Nevertheless, eosinophilic, ropey collagen bands are not seen.
Fine needle aspiration (FNA) may assist in categorizing SCL/PL, however, caution is urged as sampling limitation may lead to misdiagnosis of sarcoma. Definitive classification is best reserved for microscopic evaluation of the excised specimen.
Suggested Reading:
French CA; Mentzel T; Kutzner H; Fletcher C. Intradermal Spindle Cell/Pleomorphic Lipoma, A Distinct Subset. Am J Dermatopathol 22(6): 496-502, 2000.
Karacal N; Gulcelik N; Sapan LA; Kutlu N. Giant Pleomorphic Lipoma of the Neck. Plast Reconstr Surg 117(2): 692-693, 2006.
Sachdeva MP; Goldblum JR; Rubin BP; Billings SD. Low-Fat and Fat-Free Pleomorphic Lipomas: A Diagnostic Challenge. Am J Dermatopathol 33(5): 423-426, 2009.
Yong M; Raza AS; Greaves TS; Cobb CJ. Fine Needle Aspiration of a Pleomorphic Lipoma of the Head and Neck: A Case Report. Diagn Cytopathol 32(2): 110-113, 2005.
Thirumala S; Desai M; Kannan V. Diagnostic Pitfalls in Fine Needle Aspiration Cytology of Pleomorphic Lipoma: A Case Report. Acta Cytol 44: 653-656, 2000.
Weiss S, Goldblum J. Enzinger & Weiss’s Soft Tissue Tumors (5th ed). Philadelphia: Mosby/Elsevier Inc. 444-452, 2008.