History: A 30 year-old Caucasian woman, status-post hepatectomy for a liver malignancy, presented four years later with an enlarging 4.5 cm right-sided mass in her “new†transplanted liver. The tumor was 4.2 x 3.1 x 2.2 cm and was well-circumscribed, yellow-green, and had a central scar.
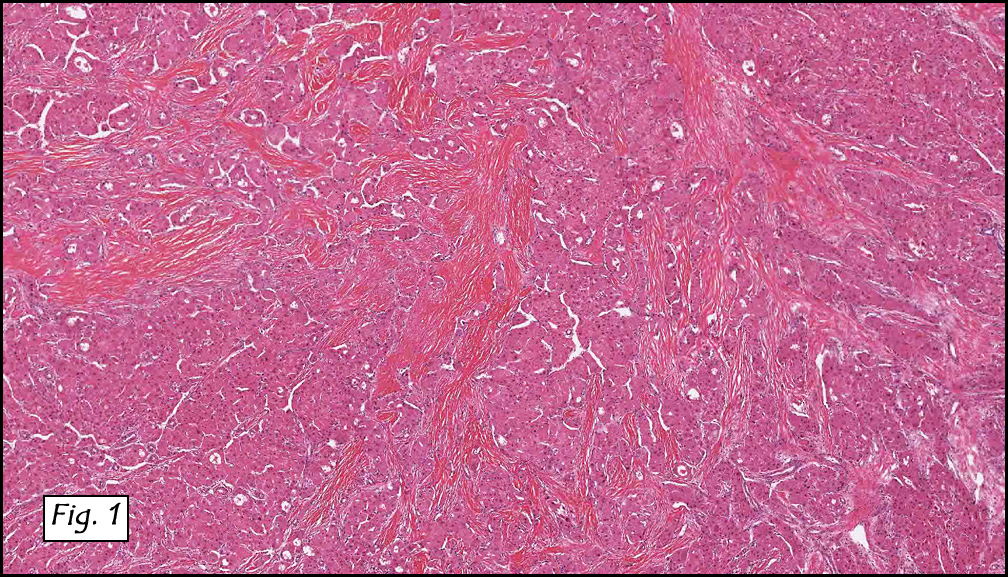
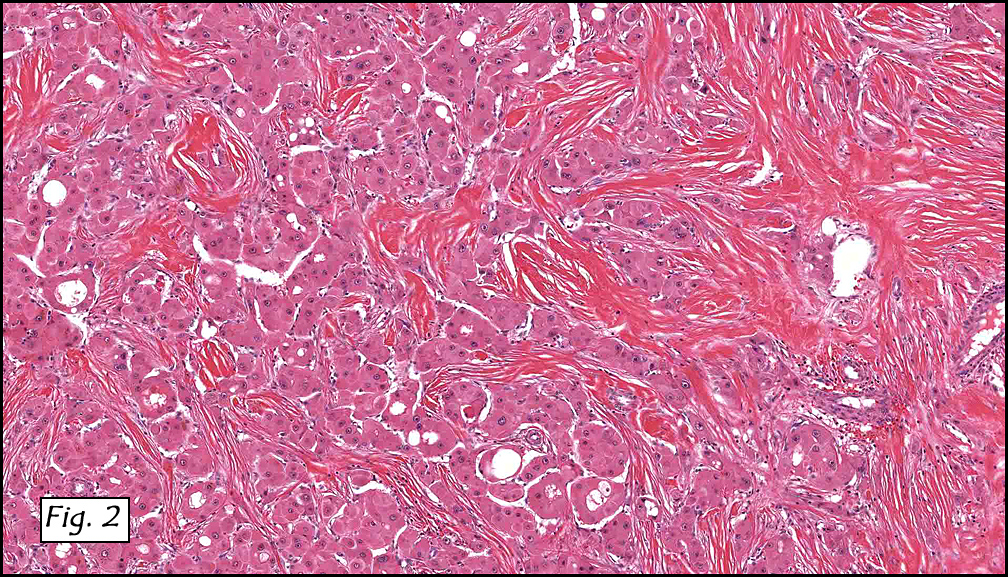
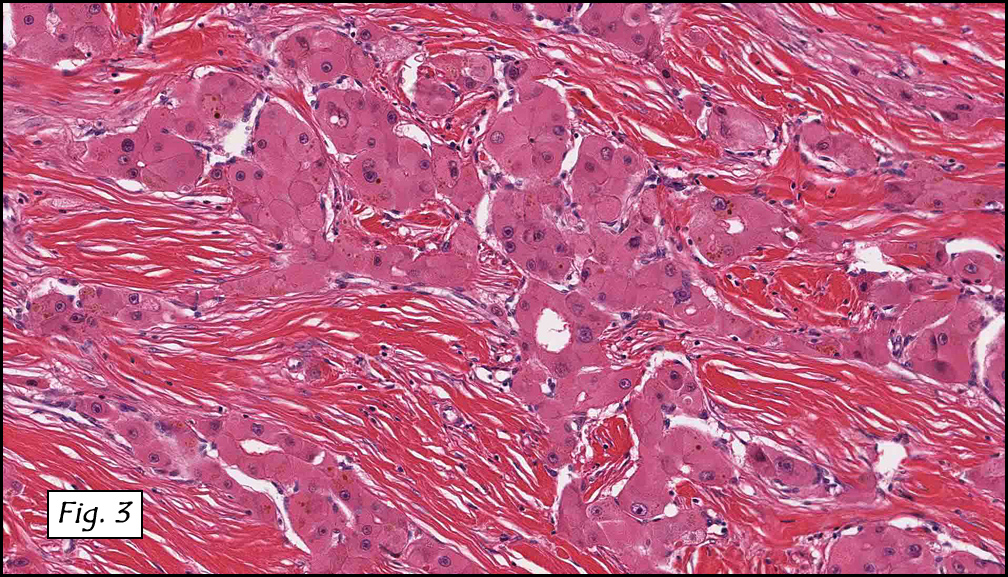
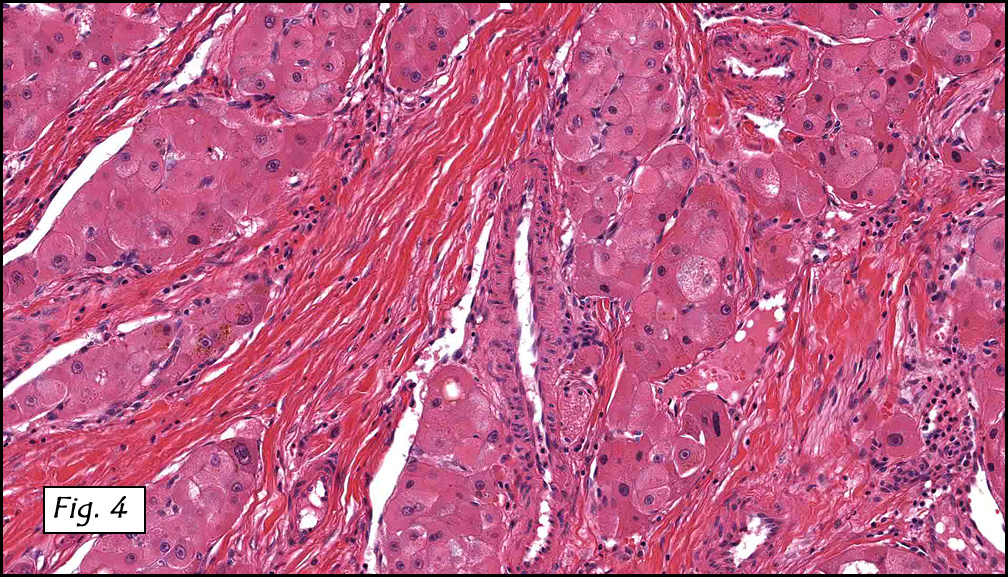
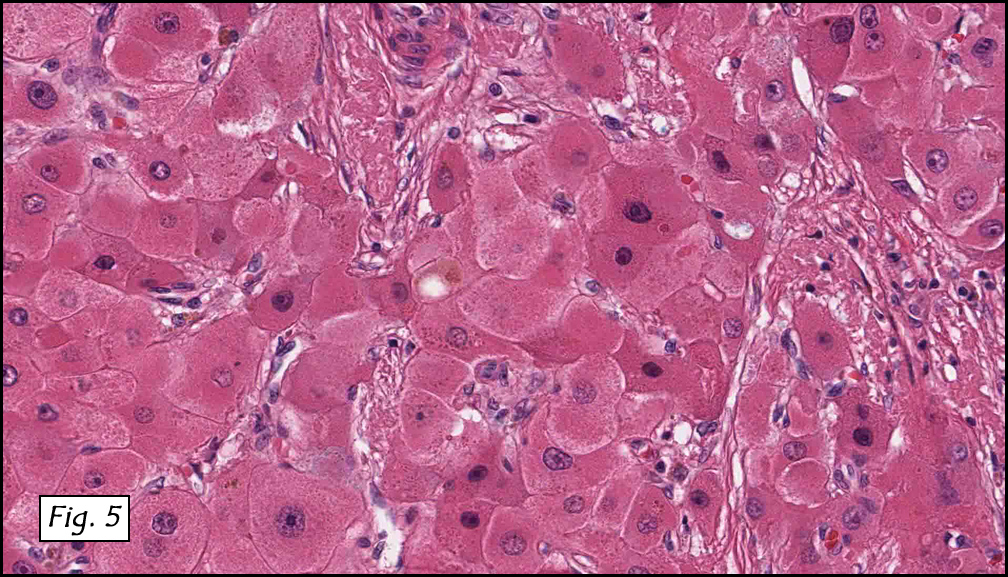
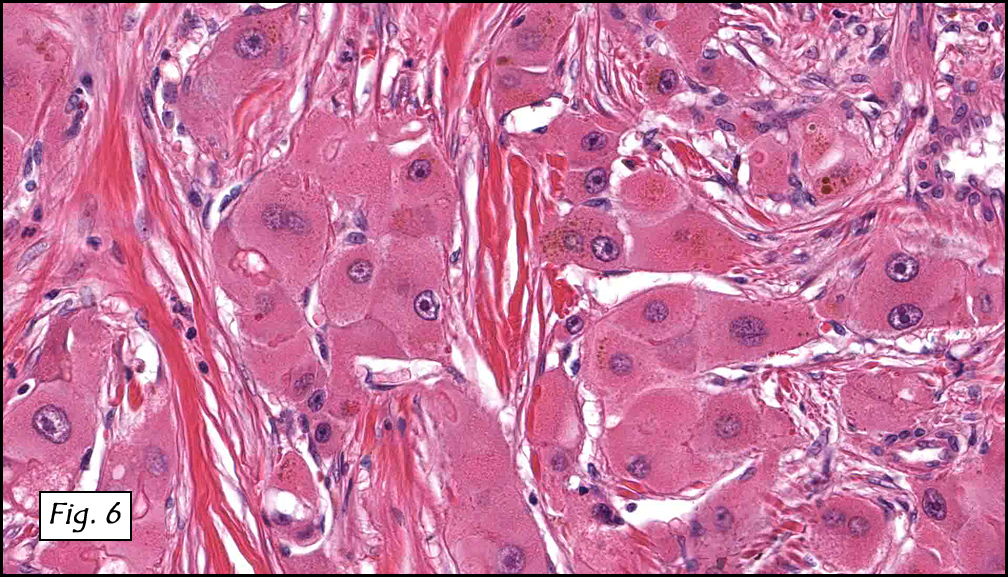
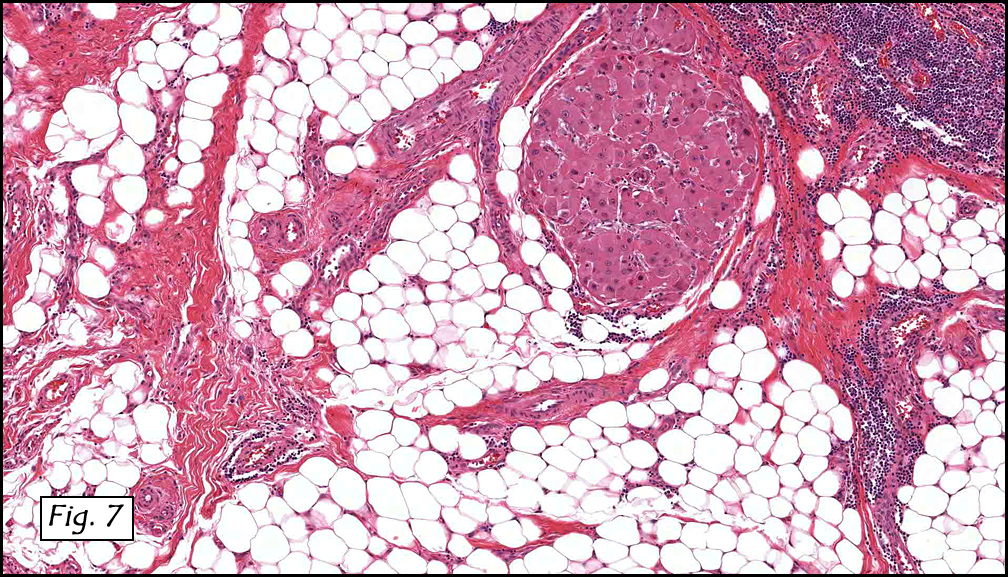
Microscopically, the tumor was solid, with prominent ramifying bands of fibrous tissue (Figs. 1, 2) which encased atypical hepatocytes arranged in medium to large-sized nests (Figs. 3, 4). The cells had large vesicular nuclei with prominent nucleoli and abundant granular eosinophilic cytoplasm (Figs. 5, 6). Bile pigment was focally present (Fig. 6). The tumor extended into perihepatic fat (Figs. 7). Neither hemorrhage nor necrosis were seen.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Hepatocellular carcinoma, fibrolamellar variant
Kate Grogan, MD, and Donald R. Chase, MD
Department of Pathology & California Tumor Tissue Registry
Loma Linda University and Medical Center, Loma Linda, California
Discussion: First described by Edmondson in 1956, fibrolamellar hepatocellular carcinoma (also known as polygonal cell type HCC) is an uncommon variant of hepatocellular carcinoma which typically occurs in young patients mean age of 26 years) who usually lack the common risk factors associated with conventional HCC. Although it was previously thought that there was a slight female predominance, current studies suggest that it occurs in equal frequency among men and women. Almost half of liver cell carcinomas in the United States occur in patients under the age of 35, and most are of this type. It is associated with a better prognosis overall than patients with HCC and cirrhosis, and the prognosis appears to be similar to that in patients with typical HCC without cirrhosis. Since it was first described, more than 180 cases have been described in the literature. Grossly, the tumors are solitary, well-circumscribed, yellow-brown and vaguely nodular. Frequently, they may have a fibrous central scar (similar to the central scar seen in focal nodular hyperplasia). Serum AFP levels are typically within normal limits.
Microscopically, the tumor consists of well-differentiated polygonal cells with abundant granular eosinophilic cytoplasm, which are arranged in nests, sheets or cords. The cytoplasm often contains pale bodies or PAS positive hyaline globules. In the background are dense acellular collagen bundles. As in other forms of HCC, tumors may also have focal acinar structures, bile, multinucleated tumor cells, copper, or fat.
Fibrolamellar carcinomas typically express both hepatic (CK 8 and 18) and biliary (CK 7, 19) cytokeratins. Recent studies have shown that expression of Hep-Par-1 and CD99 may be supportive of the diagnosis. Neuroendocrine markers may be focally positive, but they are of uncertain significance.
Cytogenetic findings: These tumors are often diploid, and overall show fewer chromosomal abnormalities than do classic HCC. Tumors with no cytogenetic abnormalities appear to behave less aggressively.
Differential Diagnosis:
• Hepatocellular carcinoma, sclerosing variant may be histologically similar, however, the tumor cells are typically smaller and pseudoglandular formation is common. Also diffuse lamellar fibrosis combined with oncocytic cellular features is not typical of usual hepatocellular carcinoma
• Cholangiocarcinoma may show glandular formation, and are usually mucin positive.
• Metastatic tumors with extensive fibrosis may mimic the collagen seen in fibrolamellar carcinoma, but is usually arranged in a more haphazard manner and lacks the directional growth characteristic of fibrolamellar carcinoma.
Complete resection of the involved lobe is the therapy of choice. When tumor is deemed unresectable, liver transplantation is an option (as in this case). The tumor metastasizes primarily to regional lymph nodes, peritoneum and lung.
Suggested Reading:
Odze R, Goldblum J. Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas (2nd edition). Philadelphia: Saunders/Elsevier Inc. 1306-7, 2009.
Liu s, Chan KW, Wang B, Qiao L. Fibrolamellar hepatocellular carcinoma. Am J Gastroenterol 2009; 104: 2617-24.
Kakar S, Burgart LJ, Batts KP et al. Clinicopathologic features and survival in fibrolamellar carcinoma: comparison with conventional hepatocellular carcinoma with and without cirrhosis. Mod Pathol 2005; 18: 1417-23.
MacSween R, Burt A, Portmann B, Ishak K, Scheuer P, Anthony P. Pathology of the Liver (4th edition). London: Churchill Livingstone/Harcourt Publishers Limited. 740-1, 2002.
Torbenson M. Review of the clinicopathologic features of fibrolamellar carcinoma. Adv Anat Pathol 2007; 14: 217-23.
Moreno-Luna LE, Arrieta O, Garcia-Leiva J et al. Clinical and pathologic factors associated with survival in young adult patients with fibrolamellar hepatocarcinoma. BMC Cancer 2005; 5: 142.