History: A 62 year-old woman underwent surgical resection of a 55 gram, 6.2 x 5.4 x 4.2 cm encapsulated right breast mass. The cut surface was tan with variably-sized pink and tan soft tissue nodules ranging from 1.0 to 2.2 cm.
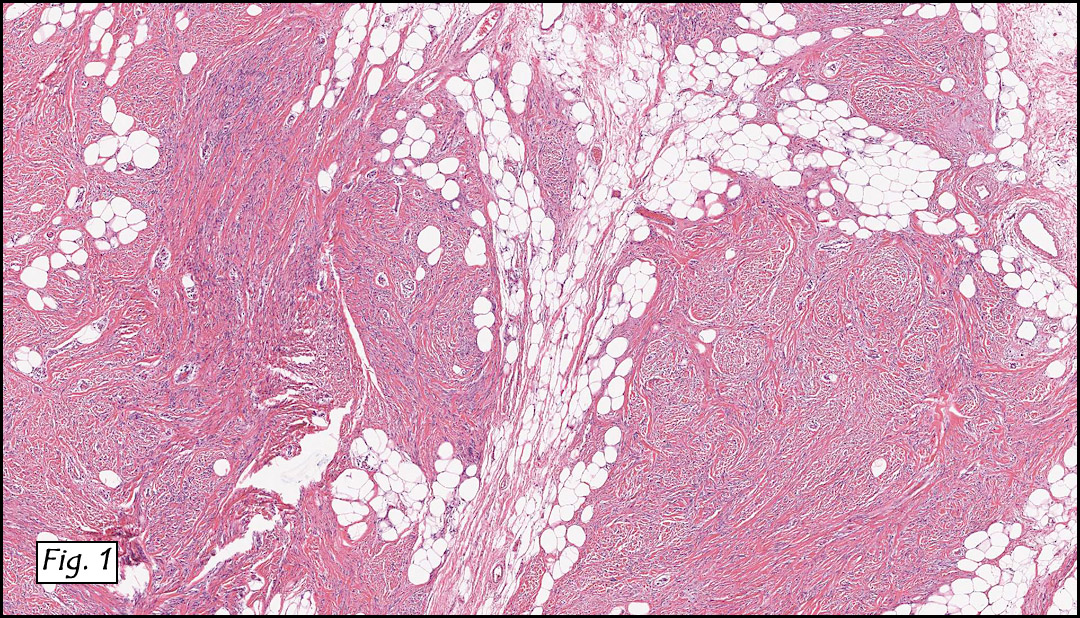
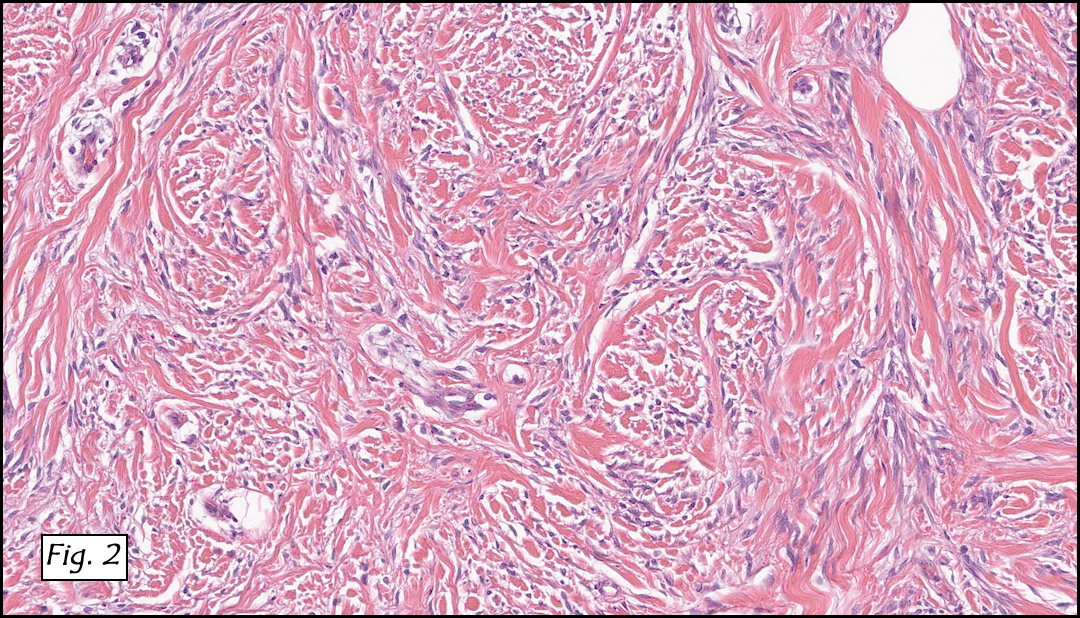
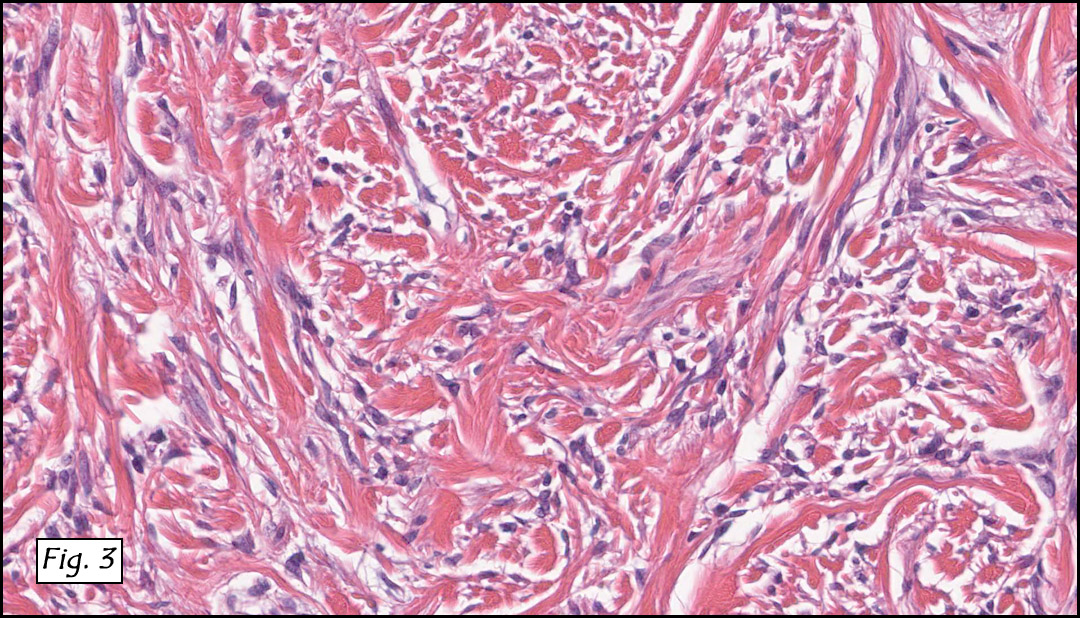
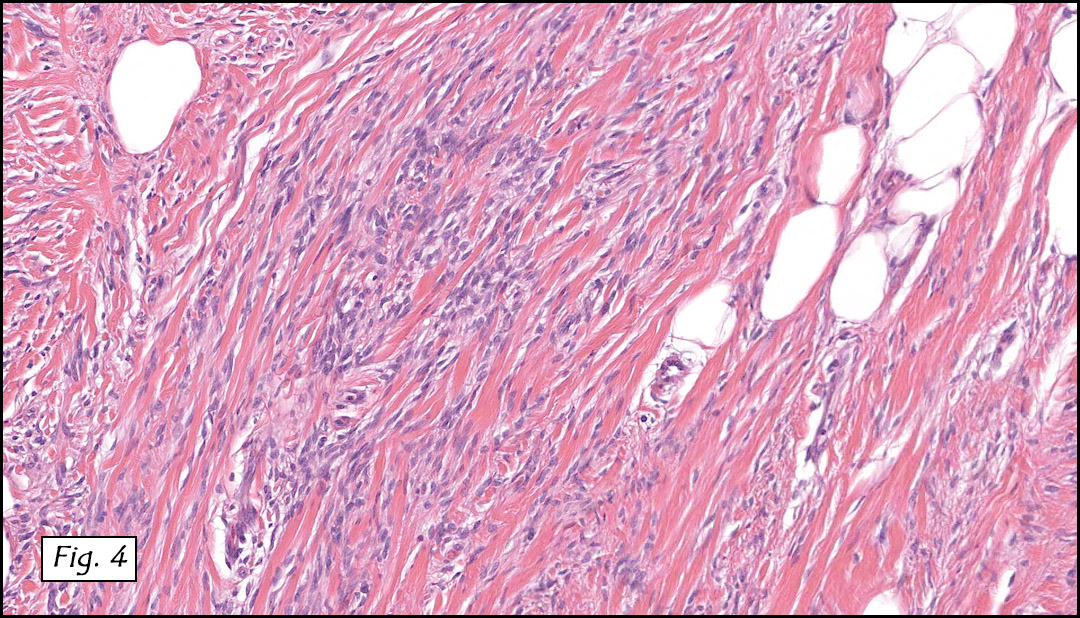
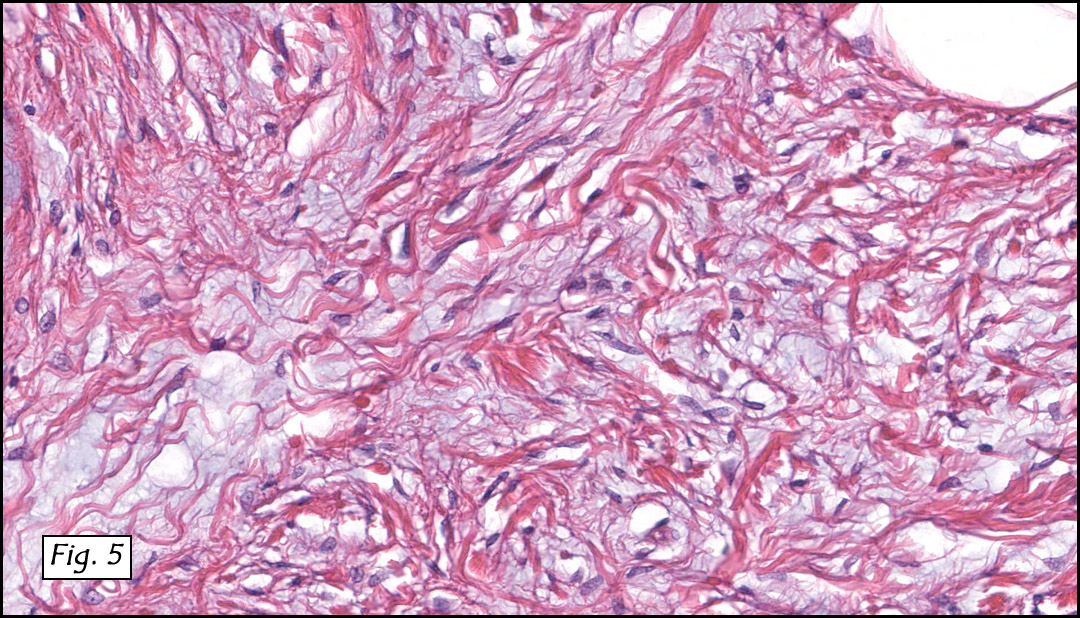
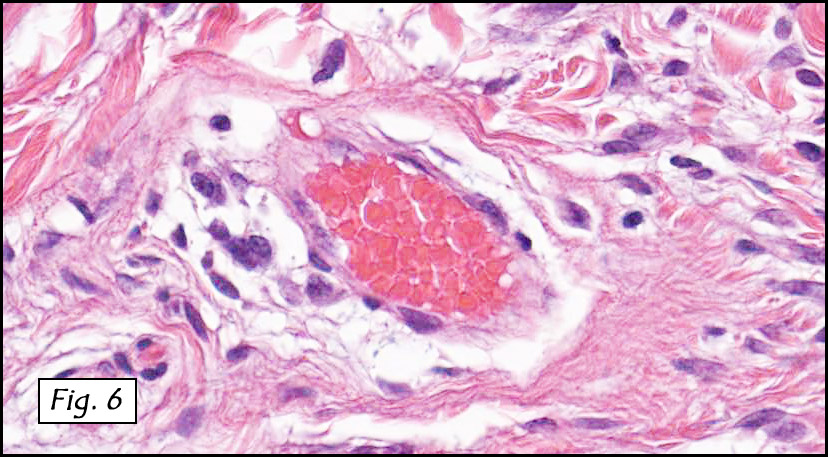
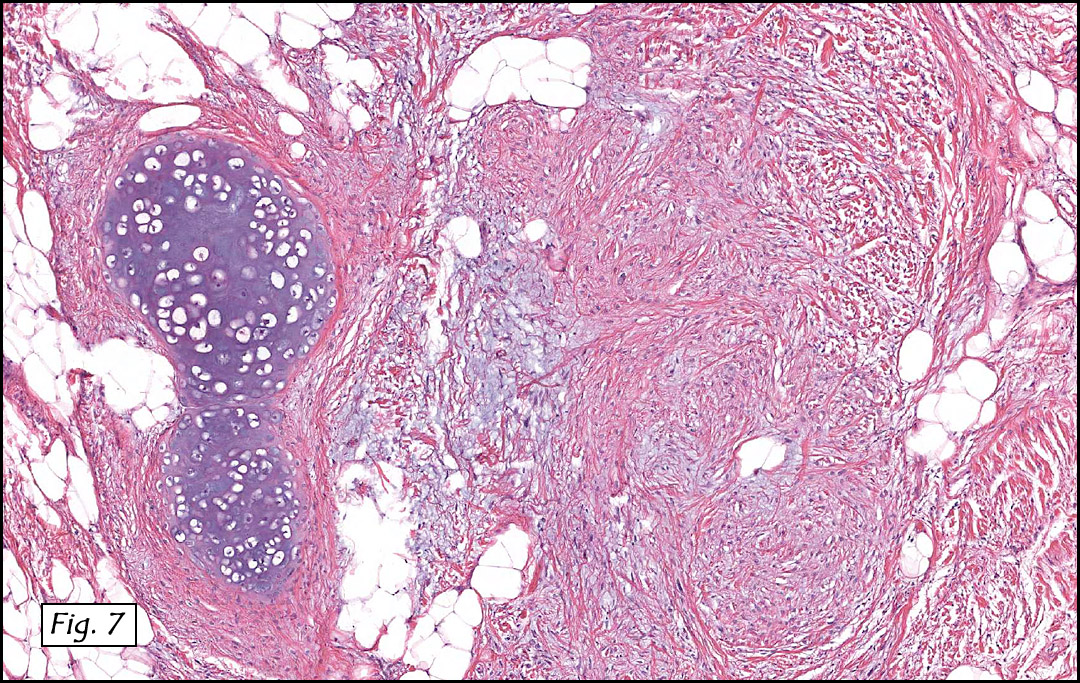
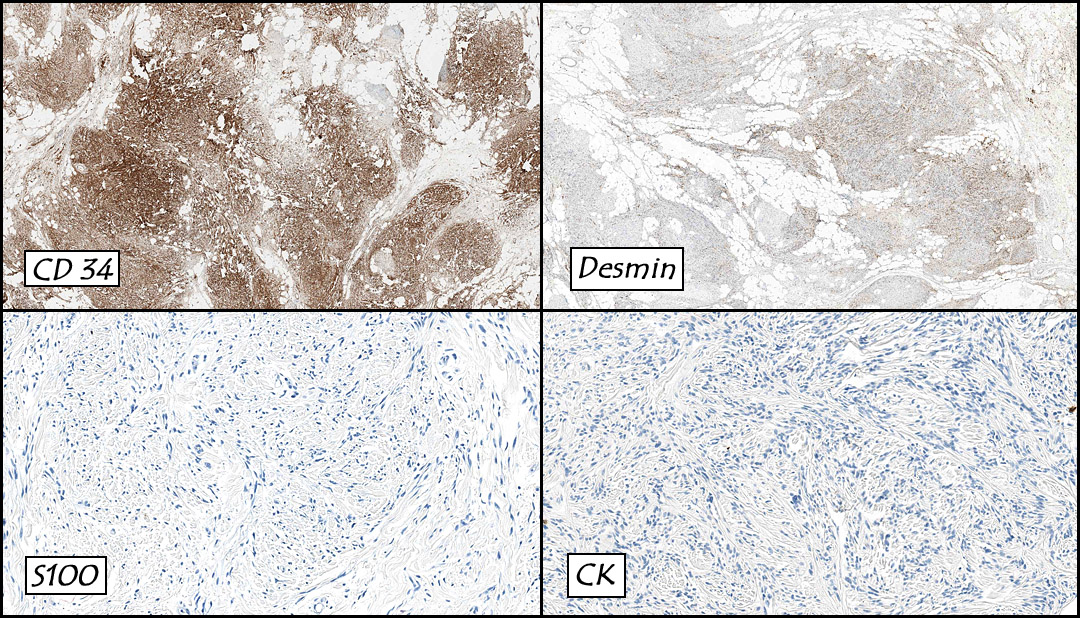
Microscopically the moderately cellular soft tissue tumor consisted of slender fibroblast-like spindle cells admixed with dense collagenous bands (Fig. 1). The cells were arranged in sheets and small fascicles which were intermixed with interweaving fibrous stroma and mature adipose tissue (Figs. 2, 3, 4). Mucoid changes were also seen (Fig. 5) as well as perivascular mast cells (Fig. 6). Chondroid metaplasia was focally present (Fig. 7). Mitoses were not increased in number and there was no evidence of significant atypia or necrosis. Immunostains showed decoration for CD31 (4+) and desmin (1+) and were negative for S100 and cytokeratin (Fig. 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Myofibroblastoma with focal chondroid metaplasiaâ€
Kate Grogan, MD, and Donald R. Chase, MD
Department of Pathology & California Tumor Tissue Registry
Loma Linda University and Medical Center, Loma Linda, California
Discussion: First described by Wargotz et al. in 1987, myofibroblastomas (MFBs) are uncommon mesenchymal neoplasms which typically occur in variably aged patients (25-85 years) with an average of 63 years. Although originally reported as having a higher incidence in men, they are currently thought to occur in equal gender frequency. They traditionally present as a well-circumscribed, mobile unilateral mass of several months duration. A single case of synchronous bilaterality has been reported. Grossly, MFBs are well circumscribed and often have a delicate fibrous psuedocapsule. The cut surface is typically gray-pink and vaguely lobular.
Microscopically, MFBs are variably cellular and are comprised of myofibroblast-resembling spindle cells which have tapered nuclei with finely dispersed chromatin, small nucleoli and a moderate amount of eosinophilic to amphophilic cytoplasm. The spindle cells often have wavy contours and are arranged in short fascicles. The stroma contains coarse bands of hyalinized collagen and conspicuous mast cells, admixed with a variable amount of adipose tissue.
Mammographically, MFBs appear as lobulated, well-demarcated and homogenous densities. Microcalcifications are absent.
The majority of cases show staining for CD34, vimentin and ER/PR. Desmin, caldesmon and androgen receptors are variably positive, and S-100 and cytokeratin are typically negative.
Cytogenetic findings: Partial monosomy 13q has been detected in two cases, as well as partial monosomy 16q in one of these two cases. Curiously, these same rearrangements are characteristic of spindle cell lipomas.
Differential Diagnosis:
• Fibromatosis of the breast typically presents as an ill-defined mass which may be associated with skin dimpling, nipple retraction and a stellate mammographic appearance. These entities will also be CD34 negative, whereas the majority of myofibroblastomas demonstrate CD34 positivity.
• Nodular fasciitis, although CD34 positive, typically demonstrates a more infiltrative pattern and has stroma that is focally pushed apart by pools of mucinous material.
• Myoepitheliomas are rare spindled lesions, which usually showing mild to moderate nuclear pleomorphism. These lesions are traditionally keratin, vimentin and EMA positive, and CD34 and ER/PR negative.
• Well-differentiated metaplastic carcinoma of the breast and stromal sarcomas usually present as ill-defined infiltrating masses, whereas myofibroblastomas are generally well-circumscribed and rarely invade adjacent breast tissue.
• Myofibroblastomas are readily distinguished from fibroadenomas due to their lack of ductal structures.
Conservative, but complete surgical excision is the treatment of choice. MFBs rarely recur and do not have metastatic potential.
Suggested Reading:
Tavassoli F, Eusebi V. Tumors of the Mammary Gland (4th edition). Washington DC: American Registry of Pathology, 2009.
Weiss S, Goldblum J. Enzinger and Weiss’s Soft Tissue Tumors (5th edition). Philadelphia: Mosby/Elsevier Inc. 535-6, 2008.
Pauwels P, Sciot R, Croiset F, Rutten H, Van den Berghe H, Dal Cin P. Myofibroblastoma of the breast: genetic link with spindle cell lipoma. J Pathol 2000; 191 (3): 282-5.
Tavassoli F. Pathology of the Breast (2nd edition). Stamford, Connecticut: Appleton & Lange. 686-691, 1999.
Magro G. Mammary myofibroblastoma: a tumor with a wide morphologic spectrum. Arch Pathol Lab Med 2008; 132(11): 1813-20.