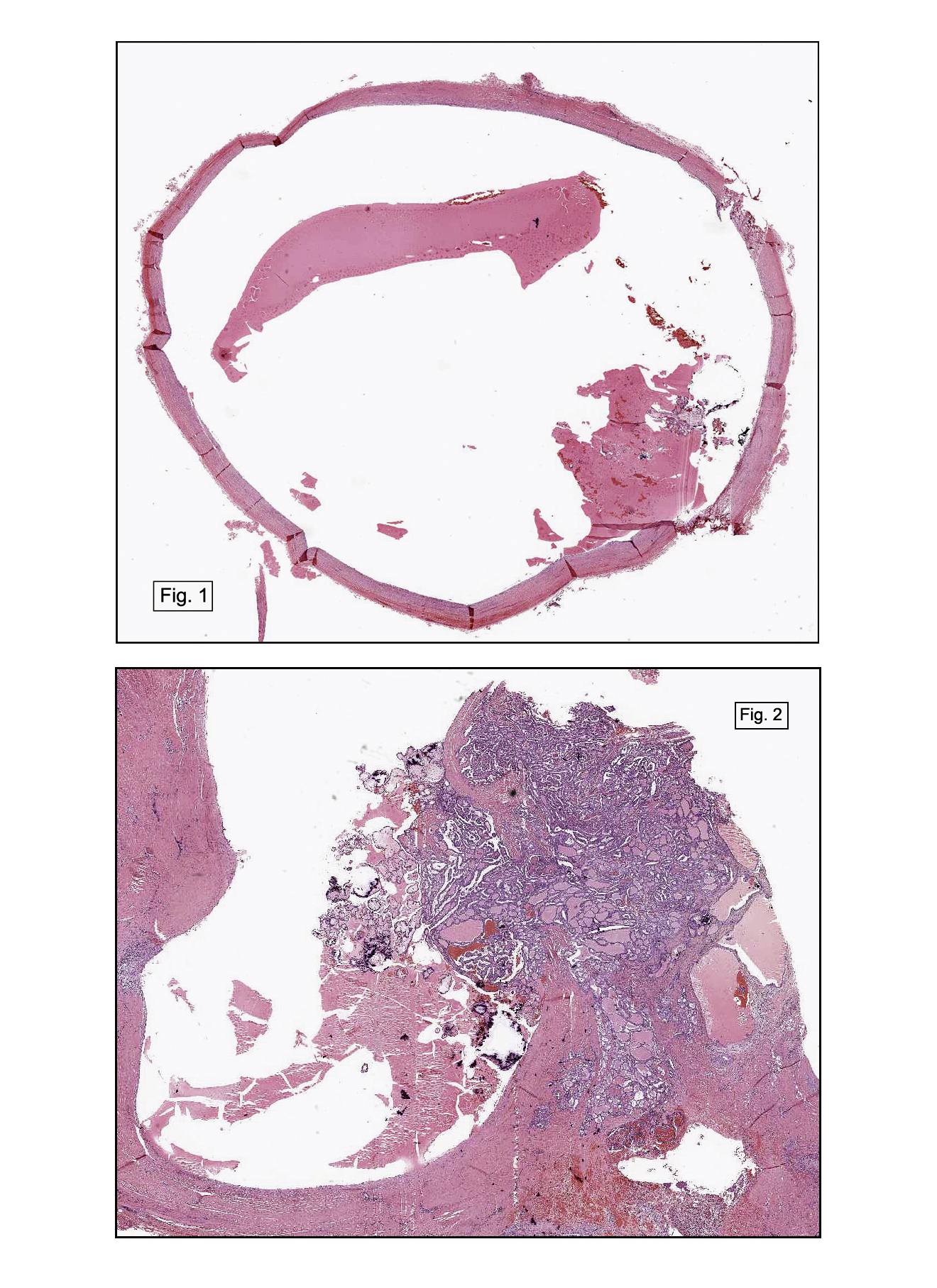
History: A 50 year old man presented with a 2 cm fluctuant midline anterior neck mass. The removed specimen was a unilocular cyst which exuded serous fluid. A papillary nodule was noted on its luminal surface.
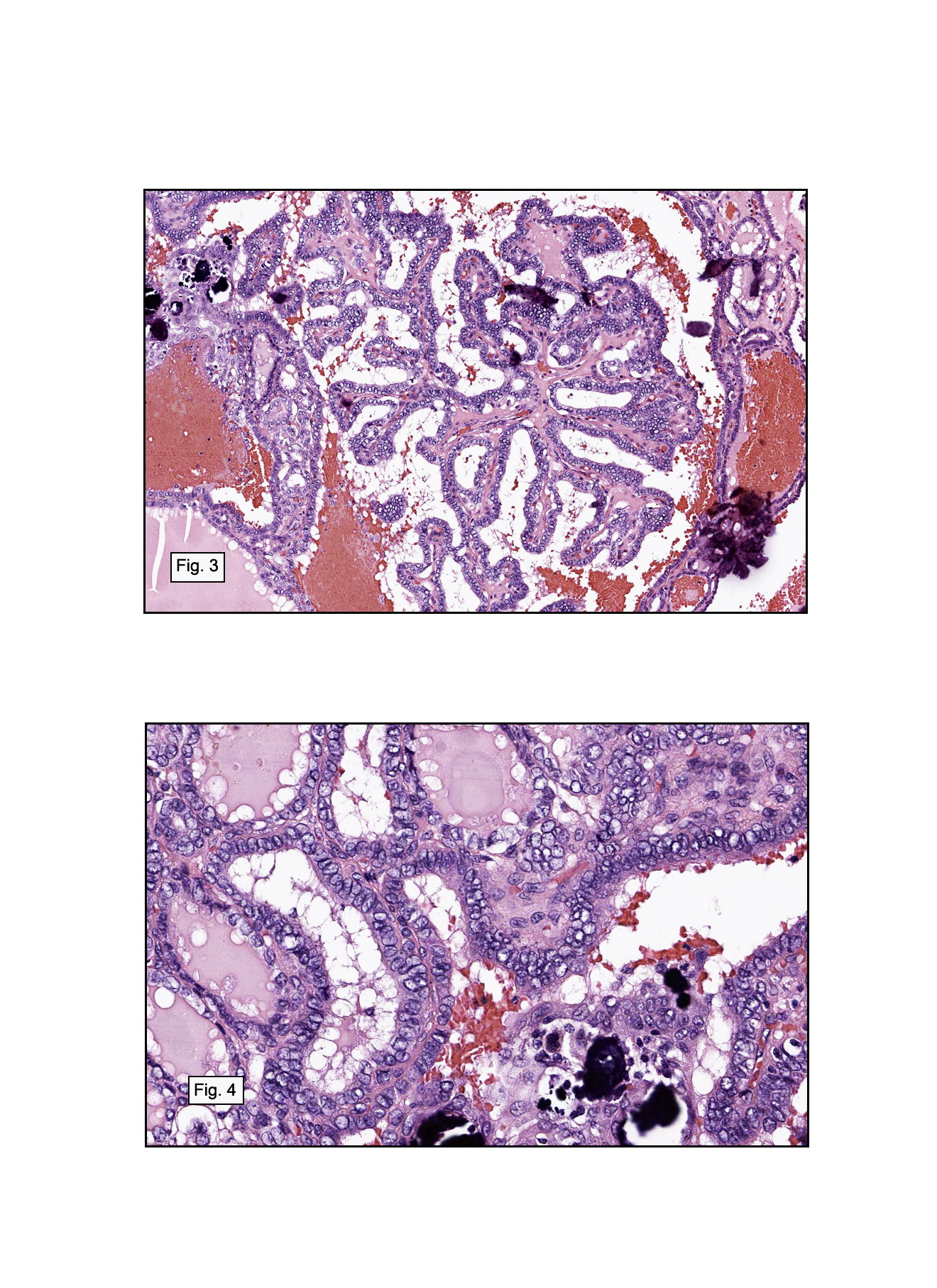
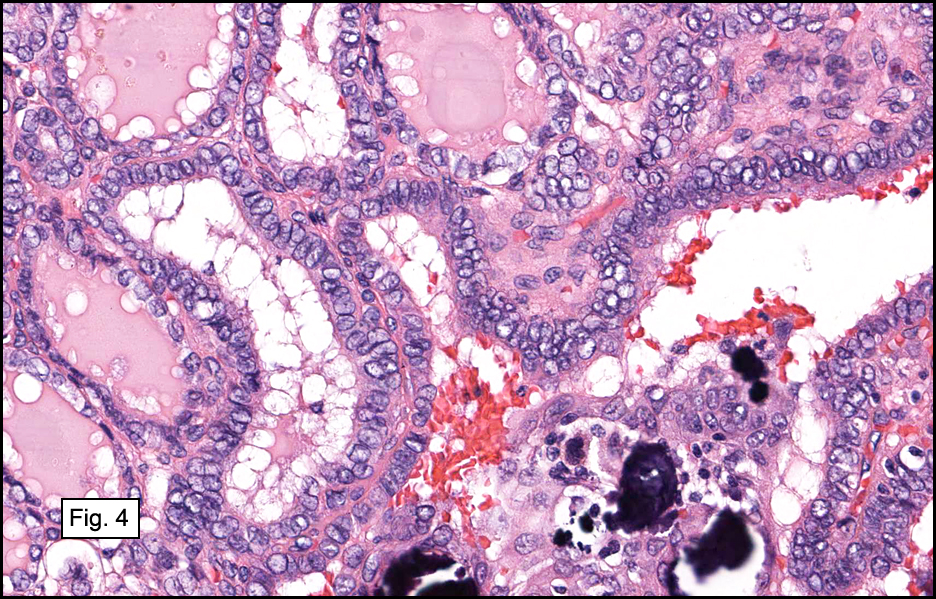
Microscopically, the cyst had a denuded epithelial lining supported by fibrous tissue with varying numbers of chronic inflammatory cells (Fig. 1). It also showed a papillary excrescence protruding into the cyst wall (Fig. 2). Tumor cells were crowded and arranged in papillary fronds and follicular patterns (Fig. 3). They had enlarged nuclei and occasional calcifications. Some showed longitudinal clefts. Nucleoli were inconspicuous and peripherally located. Many of the cells showed central cytoplasmic clearing giving the cells an “Orphan Annie†appearance (Fig. 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Classic Papillary Thyroid Carcinoma†arising in thyroglossal duct cystâ€
David Panther, MSIV, and Donald R. Chase, M.D.
Department of Pathology and Human Anatomy, Loma Linda University and Medical
Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Thyroid tissue has its embryologic origin at the foramen cecum at the base of the tongue from which it migrates into the lower anterior neck. The tract then degenerates. However, incomplete regression of this tract, can accumulate fluid and form a cyst (thyroglossal duct cyst [TDC]) usually lined with columnar epithelium. Occasionally the epithelium can undergo squamous metaplasia, or become denuded and/or inflamed. During its descent, the thyroid may leave ectopic tissue anywhere along the path and up to 60% of TDCs are associated with residual thyroid tissue. These elements are physiologically similar to those in the lower neck, however they lack parafollicular C cells. The remnant tissue can be responsible for any traditional thyroid disease, except medullary carcinoma, a tumor of C cell origin.
Rarely (<1%) residual thyroid tissue give rise to a primary malignancy, mostly papillary thyroid carcinoma (80%), (PTC). Other malignancies include follicular carcinoma and anaplastic carcinoma
Questions have been raised over the origin of PTC in a TDC, namely whether this entity represents a TDC-related primary versus a thyroid primary with local metastasis to a TDC. However, a substantial number of cases have been reported where the thyroid was removed and carefully examined. Roughly 20-50% of the lower neck thyroids have had concurrent tumor, implying that at least half of the upper neck tumors are most likely to be primary TDC tumors. In addition, occult thyroid malignancies are often found at autopsy in asymptomatic individuals, indicating that a significant portion of concurrent TDC and thyroid gland tumors are coincidental. It is generally accepted that the thyroid should not be automatically excised unless clinical evidence of a mass or abnormal scintiscan is/are present in the lower neck thyroid gland.
The differential diagnosis includes other thyroid epithelial neoplasms, as well as squamous cell carcinoma. Although metastatic disease has not yet been reported in TDCs, possible look-alikes could include metastases from clear-cell variants of lung and renal carcinoma, melanoma, and mucinous gynecologic malignancies.
– Clear Cell (“Sugarâ€) Tumor of the Lung: cells have a large cytoplasmic glycogen droplet, displacing the nucleus peripherally. In addition, it stains positive for HMB-45.
– Clear Cell Renal Cell Carcinoma: central nuclei are surrounded by clear cytoplasm, with cells often arranged in nests surrounded by branching fibrovascular tissue.
– Melanoma: features include haphazard arrangement of cells, nuclei that are pleomorphic and readily seen nucleoli and mitoses. Key immunohistochemical markers include HMB-45, MART-1, Melan A, and S-100.
– Mucinous Cystadenocarcinoma: the cyst may be multiloculated. The epithelial component may be several cells thick, with atypical nuclei containing prominent nucleoli, pale cytoplasm, and extracellular mucin. CEA is the most important immunohistochemical marker.
Suggested Reading:
DeLellis RA, Nikiforov YE. Thyroid and Parathyroid. In: Gnepp, DR. Diagnostic Surgical Pathology of the Head and Neck. Saunders Elsevier, Philadelphia, PA. 2009.
Luna MA, Pfaltz M. Cysts of the Neck, Unknown Primary Tumor, and Neck Dissection. In: Gnepp, DR. Diagnostic Surgical Pathology of the Head and Neck. Saunders Elsevier, Philadelphia, PA. 2009.
LiVolsi, VA. Surgical Pathology of the Thyroid. Volume 22 in the series: Bennington, JL, ed. Major Problems in Pathology. WB Saunders Co., Philadelphia, PA. 1990.
Hartl DM, Al Ghuzlan A, Chami L, et al. High rate of multifocality and occult lymph node metastases in papillary thyroid carcinoma arising in thyroglossal duct cysts. Ann Surg Oncol. 2009;16:2595-601.
Peretz A, Leiberman E, Kapelushnik J, Hershkovitz E. Thyroglossal duct carcinoma in children: case presentation and review of the literature. Thyroid. 2004;14:777-85.
Motamed M, McGlashan JA. Thyroglossal duct carcinoma. Curr Opin Otolaryngol Head Neck Surg. 2004;12:106-9.