History: A 34-year-old Caucasian male accountant for a powder factory and brass foundry experienced low-grade fever, debility (fatigue?), and weakness. He was found to have a slight infiltration in the right lower and mid lung fields. Cultures were negative, however he continued to have progressive dyspnea for the next two years. During that time he also developed a chronic cough productive of a copious amount of white sputum which was occasionally greenish or streaked with blood. He was admitted with severe dyspnea on exertion.
A physical examination revealed no significant findings, however the chest x-ray showed diffuse bilateral mottling in all lung areas, mostly in the lower lobes. Hemoglobin levels were slightly high at 18.2, and sputum cultures grew alpha streptococcus and staphylococcus epidermis. A left thoracotomy was performed. No pleural adhesions were noted, however the surgeons observed that the lung did not expand normally. Biopsies were taken from the left lingular segment and the left upper lobe.
Two tissue samples were examined. One was soft, fluffy, red-pink, and well aerated. The other contained firm, gray nodules up to 0.8 cm in greatest diameter.
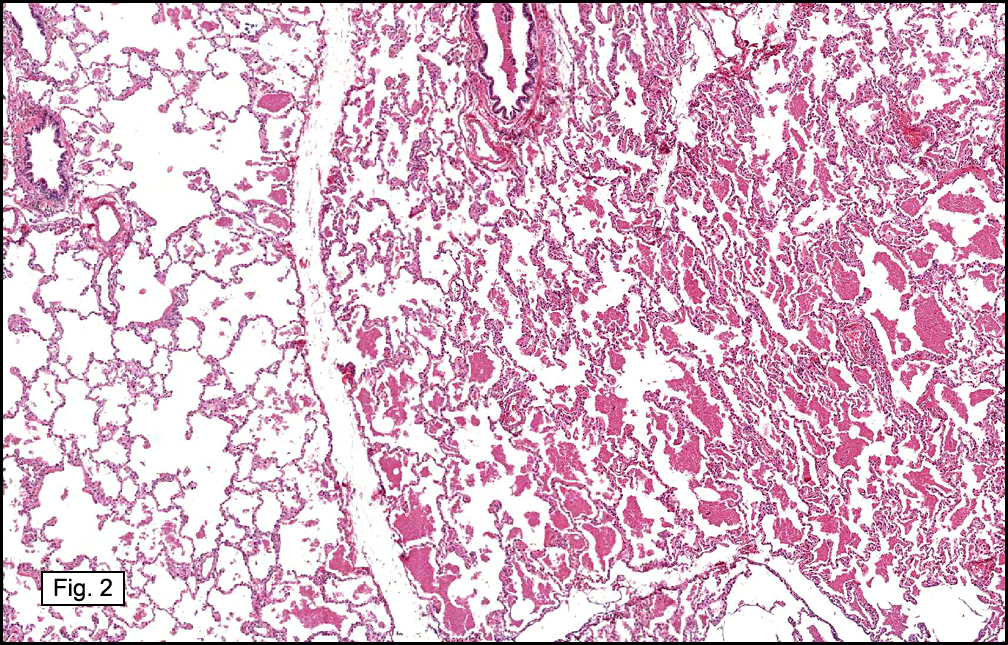
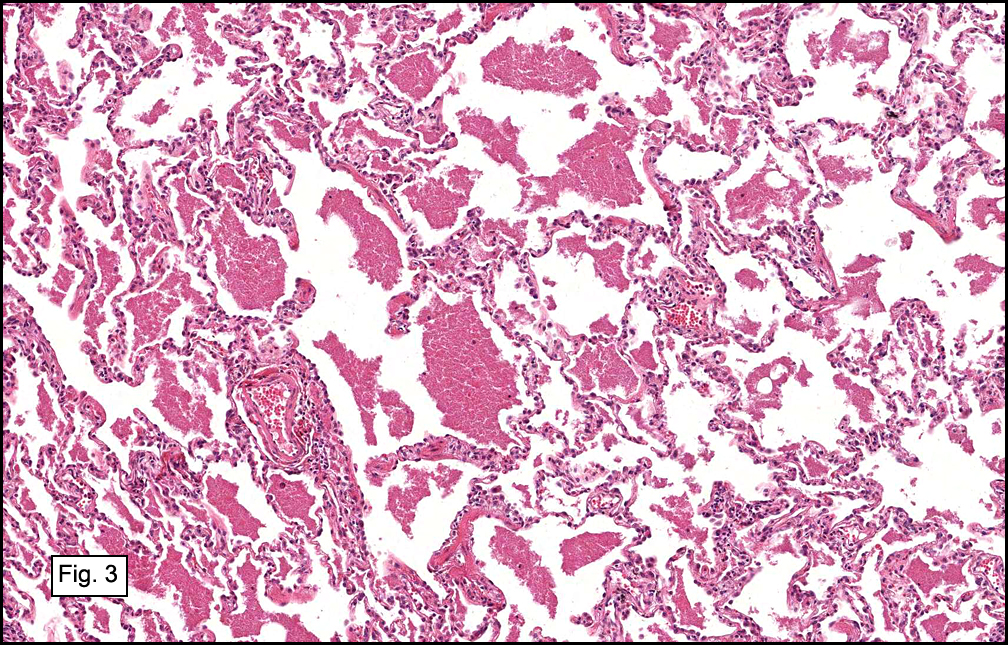
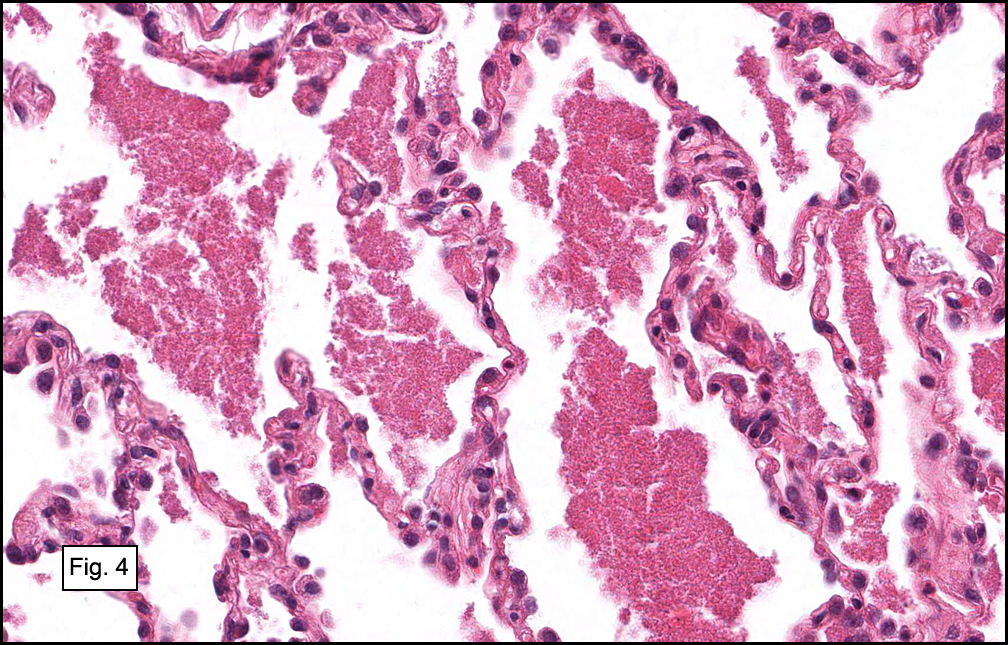
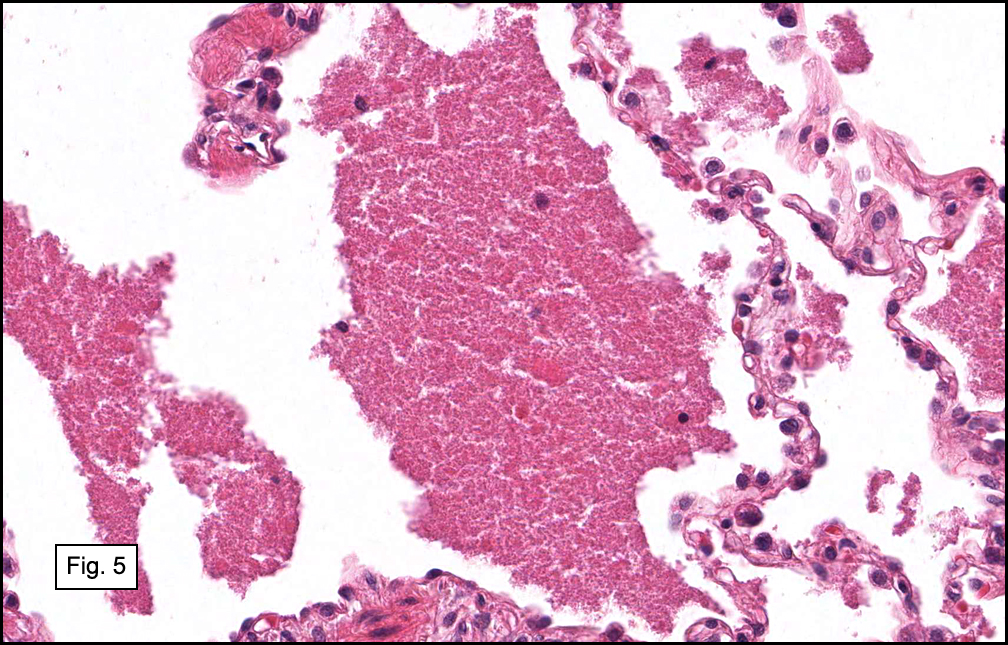
Histologic sections showed focal, nodular areas (Fig. 1) comprised of alveoli which were filled with an intensely eosinophilic material made up of tiny granules and amorphous debris (Figs. 2,3, 4, 5). These areas were immediately adjacent to essentially normal lung tissue, without a surrounding inflammatory response. No other significant abnormalities were identified.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Pulmonary Alveolar Proteinosisâ€
Christine M. Birsan M.D., and Donald R. Chase, M.D.
Department of Pathology and Human Anatomy, Loma Linda University and Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Pulmonary alveolar proteinosis (PAP) is a rare condition in which a lipid-rich, granular proteinaceous eosinophilic material fills the alveoli. “Primary†cases are found in isolation, while “secondary†PAP may occur in the setting of infection (tuberculosis, Pneumocystis jirovecii), malignancy (especially leukemia and lymphoma), immune deficiency (chemotherapy, congenital alymphoplasia, hypogammaglobulinemia, juvenile dermatomyositis), environmental dust exposure (wood, aluminum, silica, kaolin), and lysinuric protein intolerance. A history of smoking is present in many, but not all cases. Most patients present between the ages of 20-50, however 18% of cases occur in infants and children. A congenital form is described by Leslie and Wick as a lethal disease caused by defects in surfactant production and metabolism, some of which are in association with mutations of the surfactant protein B gene and genes related to secretion of surfactant proteins. “Secondary†PAP has also been observed in infants, most commonly seen with viral infections (respiratory syncytial virus, cytomegalovirus, and parainfluenza virus). “Primary†PAP is unusual in infants and children, but may be seen in adolescents. Males are affected more often than females at a ratio of approximately 2:1-4:1, and the disease may be more common in Caucasians.
The pathogenesis of PAP is unknown. Studies have suggested that macrophage dysfunction may play a role, in which there is a reduced ability to process surfactant (a significant component of the accumulated intra-alveolar material). Mutant mice lacking the gene for granulocyte-macrophage-colony-stimulating factor (GM-CSF) develop a similar disease process which is reversed when GM-CSF is replaced. In addition, antibodies against GM-CSF have been discovered in human cases of PAP (especially “primary†PAP), further supporting this hypothesis. Alternatively, defective production of surfactant may be a consideration, as the pathologically accumulated surfactant lacks its usual surface-active properties, while surfactant extracted from uninvolved areas of the patient’s lung shows normal activity. It has been shown experimentally that the material from PAP produces macrophage dysfunction in normal human blood monocytes and reduces activity of lymphocytes, raising the possibility that the macrophage dysfunction may be a secondary result rather than a primary cause. The wide variety of clinical situations in which this process is observed suggests that PAP represents a common tissue reaction to a broad range of insults.
Clinically, the onset of PAP is often insidious. About one-third of patients are asymptomatic at presentation despite having extensive radiologic abnormalities. Patients who are symptomatic may have a nonproductive cough, a cough productive of chunky, gelatinous material, and/or streaky hemoptysis. Dyspnea on exertion, fatigue, weight loss, chest pain, and low-grade fever may also be present. Occasionally clubbing and cyanosis are observed. Crackles are sometimes heard on auscultation however they are often absent.
Radiographic findings usually include bilateral and symmetric areas of vaguely nodular airspace consolidation or hazy ground-glass opacity. Peri-hilar regions and lower lobes are most severely affected. Interlobular septal thickening and ground-glass opacities seen on CT scans produce a characteristic “crazy paving†appearance. This pattern, although suggestive of the diagnosis, is also seen in other conditions.
Pulmonary function testing most commonly demonstrates a restrictive process, and a decrease in the diffusion capacity for carbon monoxide (DLCO) out of proportion to the reduced lung volume is sometimes seen. Hypoxemia and compensated respiratory alkalosis are frequent and are made worse by exercise. An elevated shunt fraction is usually present.
Lab values may reveal polycythemia, hypergammaglobulinemia, and increased lactate dehydrogenase. Serum levels of lung surfactant proteins A and D (SP-A, SP-D) have been found to be markedly high which can help narrow the diagnosis, however, other lung processes can have similar findings. Elevated levels of several tumor markers have been identified in the BAL fluid from some patients, including carcinoembryonic antigen (CEA), carbohydrate antigens sialyl Lewis (CA19-9), and sialyl SSEA-1 (SLX). KL-6, a mucin-like glycoprotein may also be useful for diagnosis when found in serum or BAL specimens. Cultures may reveal Nocardia or other opportunistic mycobacterial, fungal, and viral agents thought to represent secondary infection.
Cytologic preparations may suggest the diagnosis of PAP. In BAL specimens, abundant lipoproteinaceous material causes an opaque appearance, and large, acellular eosinophilic bodies may be seen in a background of eosinophilic granules. PAS-positive proteinaceous material as well as macrophages engorged with PAS-positive material point to the diagnosis.
Tissue examination is frequently necessary for definitive diagnosis. Grossly, lung tissue is heavy and viscid, containing yellow fluid which leaks from cut surfaces. Firm, yellowish-white nodules scattered throughout the parenchyma range from a few millimeters to 2 cm. Microscopically, eosinophilic proteinaceous granular material fills the alveoli and occasionally involves bronchioles and alveolar ducts, leaving the interstitial architecture of the lung generally intact. A diffuse pattern is usually seen, however focal or patchy involvement also exist, as seen in this case. Hyperplastic, cuboidal, type 2 pneumocytes are often line the alveolar septae. Sharply demarcated round, empty spaces, cholesterol clefts, and small, dense, globular eosinophilic clumps are distinctive findings within the accumulated material which may also contain cellular debris, foamy macrophages, ghosts of degenerated cells, and detached type 2 pneumocytes. It is usually PAS-positive and diastase-resistant, while staining for antibody to surfactant apoprotein may be positive especially in “primary†disease. Alcian and mucicarmine stains are negative. Frozen sections shows abundant lipid, highlighted with Oil Red O staining. Examination by electron microscopy demonstrates concentrically laminated myelin figures and lamellar bodies within the proteinaceous material which look identical to the cytoplasmic inclusions of type 2 pneumocytes, suggestive of surfactant. Polarization microscopy may reveal birefringent needle-like particles if there has been an exposure to dust. Interstitial fibrosis or inflammation are typically not prominent and if present may indicate an associated infection, but may also indicate long-standing or recurrent PAP.
The differential diagnosis for PAP includes pulmonary edema, alveolar mucinosis, and Pneumocystis jirovecii pneumonia. Pulmonary edema and alveolar mucinosis lack the granularity of PAP, as well as the intense eosinophilic staining, cholesterol clefts, and engorged macrophages containing PAS-positive debris. The intra-alveolar exudate seen in Pneumocystis jirovecii may be distinguished from PAP by the cysts or organisms which appear as “bubbles†within the eosinophilic material which stain positive for Gomori methenamine silver (GMS).
Treatment for PAP should be initiated when the patient becomes sufficiently symptomatic, as many patients have little or no impairment and spontaneous remission may occur. Severe dyspnea and hypoxemia at rest or with exercise warrant therapeutic whole lung lavage via a double-lumen endotracheal tube, the most widely accepted and effective treatment. Patients often feel dramatically better after this treatment, although potential complications include malpositioning of the endotracheal tube, saline spillover into unlavaged and ventilated lung, and hydropneumothorax. Thirty to forty percent of patients require lavage only once, while some patients require repeat lavages at intervals of 6 to 12 months. Corticosteroids or other immunosuppressives should not be used, as there is concern that they may increase mortality by aggravating or inducing secondary opportunistic infections. Further study is necessary to determine the potential use of GM-CSF as a therapeutic option.
Suggested Reading:
Travis W, Colby T, Koss M, et al. Non-neoplastic disorders of the lower respiratory tract. In King D, ed. Atlas of Nontumor Pathology. Washington, DC: American Registry of Pathology, Armed Forces Institute of Pathology; 2002.
Katzenstein AL III. Katzenstien’s and Askin’s Surgical pathology of non-neoplastic Lung disease. 3rd edition. Philadelphia, PA: WB Saunders Company; 1997.
Hammar S. Pleural diseases. In: Dail D, Hammar S, eds. Pulmonary Pathology. 2nd ed. New York, NY: Springer-Verlag; 1994.
Leslie K, Wick M. Practical pulmonary pathology. A diagnostic approach. 1st edn. Philadelphia: Churchill-Livingstone; 2005.