 History: A 25 year old man with a 1 cm nodule in his arm had an excisional biopsy.
History: A 25 year old man with a 1 cm nodule in his arm had an excisional biopsy.
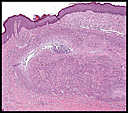
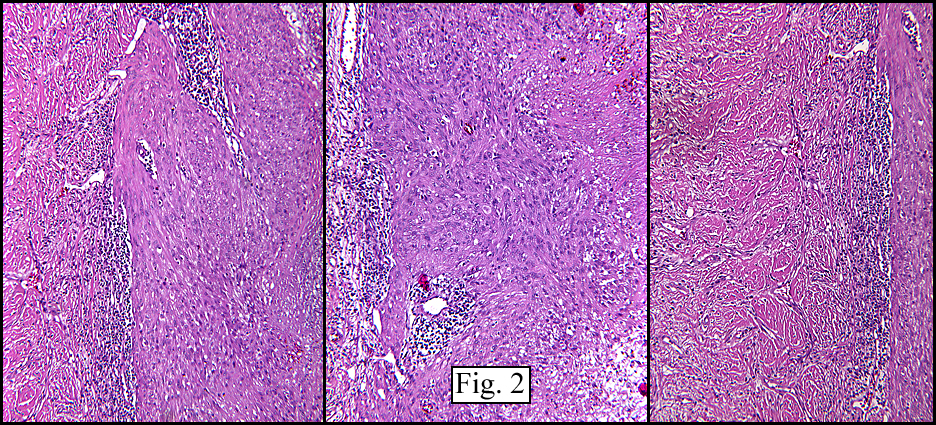
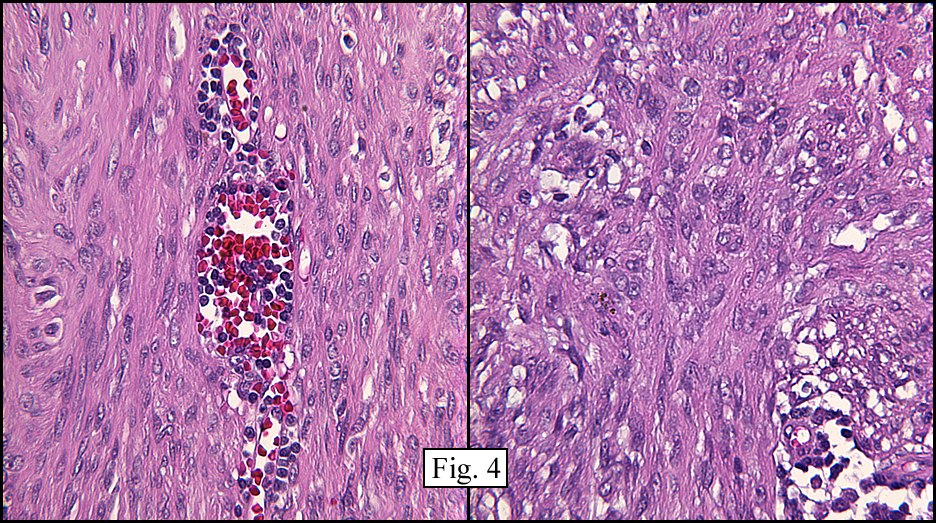
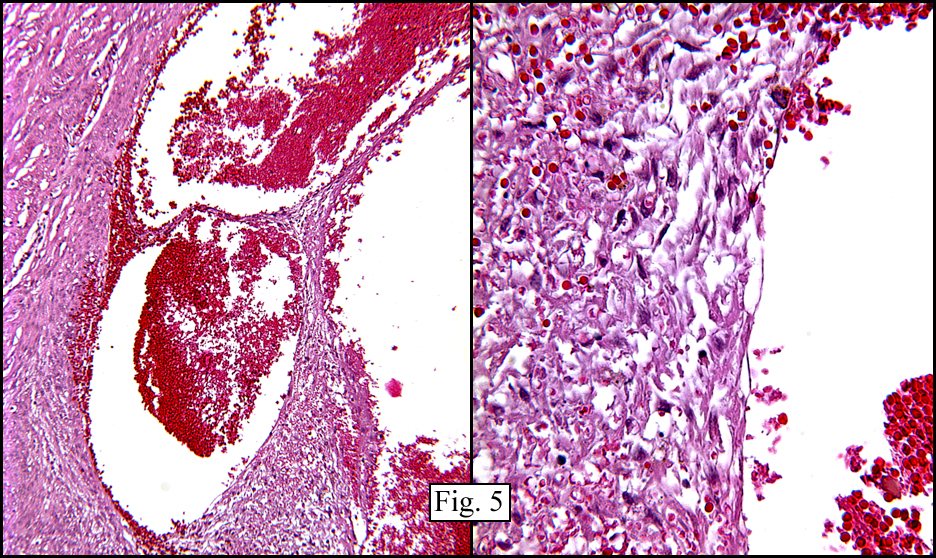
The superficial dermis resembled a simple acrochordon however the deeper dermis had sheets and nodules of spindled cells arranged in short fascicles (Figs. 1,2) These fusiform cells had ovoid nuclei and tapered eosinophilic cytoplasm (Figs. 3,4). At the periphery was a cuff of lymphocytes. There were also cystic spaces filled with erythrocytes (Fig. 5). Hemosiderin pigment was focally evident.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Angiomatoid Fibrous Histiocytoma of Armâ€
Melissa Skaugset PSF, Donald R. Chase, MD
Department of Pathology, Loma Linda University and Medical Center
California Tumor Tissue Registry
Discussion: Fibrous histiocytomas (FH) may be subdivided into two general categories based upon behavior, either benign or intermediate. The benign or cutaneous FH (a.k.a. ‘dermatofibroma’) is a solitary indolent neoplasm that generally occurs in early to middle adulthood. Histologically, FHs consist mostly of fibroblastic elements which grow in fascicles many times assuming a storiform configuration. Multiple variants of benign FH have been described, including:
Cellular
• Increased cellularity
• Decreased storiform pattern
• Mitotic activity higher, averaging 3/HPF
• Subcutaneous extension more common
Epithelioid
• >1/2 of cells are rounded/epithelioid
• Freq. areas of conventional FH appearance
• S100 negative
Aneurysmal
• Blood filled spaces lacking endothelial lining
• Abundant hemosiderin
• May have mitotic activity near hemorrhage
Clear cell
Translucent clear cell change of cells
Eruptive
Associated with HIV and SLE
Myxoid
Extensive myxoid change
Lipidized
Lipidization
Granular
Granular cell changes
Angiomatoid fibrous histiocytoma (AFH) is felt to be somewhat more aggressive than traditional forms of FH and has been given an intermediate malignant potential designation. First felt to be in the family of MFH, it was originally termed “angiomatoid MFH†but a reassessment in 1994 showed the tumor to usually be small, superficially located and to occur in a younger population than MFH. It was also shown to have limited capacity for distant metastasis. The “malignant†designation was dropped and the tumor was renamed AFH.
AFH most often arises in children, adolescents, or young adults (mean age of 20 years), though cases have been described in neonates and in the elderly. The extremities are usually involved. Two-thirds involve areas where lymph nodes may be palpated, particularly the antecubital fossa, popliteal fossa, axilla, inguinal area, supraclavicular fossa, and neck.
Patients usually present with a palpable, painless slow-growing mass, however some may present with systemic manifestations such as fever, anemia, and/or weight loss, likely due to cytokine production by the tumor.
AFH usually is described as a firm, well-circumscribed mass, several centimeters in greatest dimension (range 0.7-12 cm, mean ~ 2 cm), with blood filled cystic spaces that may be large enough to be grossly apparent and even mimic a hematoma. Depending upon the amount of hemorrhage and hemosiderin deposition it is seen to be gray to red-brown.
Microscopically, AFH consists of nodules and/or sheets of eosinophilic spindled or epithelioid cells with ovoid vesicular nuclei. Cystic spaces without endothelial lining cells are usually seen throughout as ‘pseudoangiomatoid spaces’. A cuff of inflammatory cells, mostly lymphocytes with occasional plasma cells, is characteristic as is a compressed periphery of collagen which forms a fibrous pseudocapsule.
Immunohistochemistry shows 50% positivity for desmin and surprisingly 40% positivity for EMA. Many AFHs are CD68 positive. The tumor is uniformly negative for CD21, CD35, S100, HMB-45, keratins and vascular markers.
The differential diagnosis prominently includes aneurysmal fibrous histiocytoma, a subtype of benign FH that is histologically similar to AFH. Aneurysmal FH, however, lacks the characteristic cuff of lymphocytes found in angiomatoid FH. It also lacks desmin reactivity and doesn’t present with systemic manifestations. There is, however, a possibility that the two tumors are related and may be a part of a spectrum of the same tumor entity.
AFH is an indolent tumor with a 10% local recurrence rate and a 1-2% metastatic rate (generally non-fatal to local lymph nodes), however rare cases have resulted in deaths due to late distant metastases. Local recurrence is more frequent in cases showing infiltrating margins and/or head/neck or deep intramuscular locations. No factors have been found to predict metastatic potential. With wide local excision the prognosis for AFH is excellent.
Suggested Reading:
Daw, Billups, Pappo, Jenkins, Mahmoud, Krasin, Rao. Malignant Fibrous Histiocytoma and Other Fibrohistiocytic Tumors in Pediatric Patients. Cancer. 97: 2839-47, 2003.
Fletcher, Christopher D.M., MD. Diagnostic Histopathology of Tumors, 2nd Ed. Churchill Livingstone, 2000.
Fletcher, Christopher D.M., Unni, K. Krishnan, Mertens, Fredrick. WHO Classification of Tumours: Pathology and Genetics of Tumours of Soft Tissue and Bone, 2002 Ed. IARC Press, International Agency for Research on Cancer, 2002.
Miettinen, Markku, MD. Diagnostic Soft Tissue Pathology. Churchill Livingstone, 2003.
Weiss, Sharon W., MD; Goldlum, John R., MD. Enzinger and Weiss’s Soft Tissue Tumors, 4th ed, Mosby, Inc., 2001.